The Importance of Force Couples In our Shoulders
by Tyler Tice, PT, DPT, MS, ATC
Force couples are when 2 or more muscles on opposing sides of a joint work together to provide joint stability or create movement. In the shoulder joint, there are three important force couples that help move and control our shoulders. When these force couples are not working properly, it can lead to pain and injury.
Force couples are when 2 or more muscles on opposing sides of a joint work together to provide joint stability or create movement. In the shoulder joint, there are three important force couples that help move and control our shoulders. When these force couples are not working properly, it can lead to pain and injury.
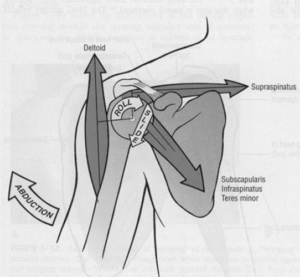
1. Deltoid-rotator cuff force couple:
- Produces largest amount of force
- Rotator cuff muscles: supraspinatus, infraspinatus, teres minor, subscapularis
- When raising arm overhead, the deltoid causes an UPWARD and OUTWARD force on the humerus (upper arm bone) during the first part of the motion
- 3 of the rotator cuff muscles (infraspinatus, teres minor, subscapularis) collectively create a DOWNWARD and INWARD force on the humerus to maintain the proper positioning of the ball in its socket.
- The supraspinatus creates a compressive force to help keep the humerus in proper positioning. When rotator cuff muscles are not working properly, this can cause greater amount of UPWARD and OUTWARD movement at the shoulder potentially causing more pressure on the humeral head as well as potentially leading to injury of other shoulder structures
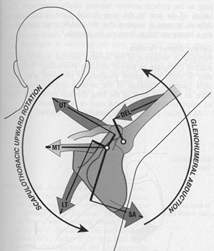
2. Upper trapezius and serratus anterior force couples
- To produce upward rotation of the scapula, or shoulder blade when raising our arms
- 4 major muscles: Serratus anterior, Lower trapezius, Upper Trapezius, Levator Scapula
- 4 important functions: Allows for rotation of the shoulder blade to keep the glenoid (socket of the shoulder) in proper positioning; Maintains proper length-tension relationship for the deltoids; Prevents impingement on the rotator cuff muscles; Provides stable scapular base for proper muscular recruitment
- Collectively, these 4 muscles act on the shoulder blade creating forces at different aspects of the shoulder blade in different directions where the end result becomes UPWARD ROTATION of the shoulder blade
- The serratus anterior and lower trapezius are the primary stabilizers of the shoulder blade when the arm is raised 90 degrees or more out to the side
- We need proper shoulder blade upward rotation to maintain shoulder stability when raising our arm to the side. It has been shown with shoulder impingement syndrome that there is decreased activity of serratus anterior, delay in activating lower trapezius, and overactivity of upper trap and levator scapula.
3. Anterior-posterior rotator cuff force couples
- Anterior (front) rotator cuff: subscapularis
- Posterior (back) rotator cuff: infraspinatus and teres minor
- Create a DOWNWARD stability within shoulder and contribute to compressive forces to maintain the humeral head within the socket when elevating arm
- Subscapularis (front) and infraspinatus (back) pull DOWNWARD and INWARD at about 45 deg angle; teres minor (back) pull DOWNWARD and INWARD at about 55 deg angle to keep shoulder centered in joint
- It is common that the shoulder internal rotator muscle groups, which includes the subscapularis are more developed compared to the teres minor and infraspinatus creating a potential force couple imbalance leading to potential lack of stability.
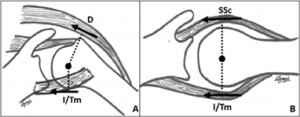
(picture on right demonstrates this)
Reference:
Ellenbecker T, Manske R, Kelley, M. Current Concepts of Orthopaedic Physical Therapy: The Shoulder: Physical Therapy Patient Management Using Current Evidence. 4th Edition. Orthopedic Section, APTA 2016