by ptfadmin | Mar 2, 2026 | Health Tips
Reviewed by Tyler Tice, PT, DPT, OCS, ATC
Background:
- Unilateral vestibular hypofunction( UVH) : partial or complete loss of function in one of the peripheral vestibular organa, and/or nerves
- Acute UVH: most commonly due to vestibular neuritis, but also may be due to trauma, surgical transection, ototoxic meds, or Meniere’s disease.
- Bilateral vestibular hypofunction (BVH): idiopathic in 20-51% of cases
- Common presentation/symptoms:
- dizziness, imbalance, and/or oscillopsia, gaze and gait instability, and impaired navigation and spatial orientation
- Spatial navigation impairments
- Memory, executive function, attention
- Prevalence increases with age
- Higher fall risk
- Typically, bilateral
Population:
vestibular hypofunction
Strong evidence:
Vestibular PT to mitigate symptoms and improve postural stability, gaze, and function
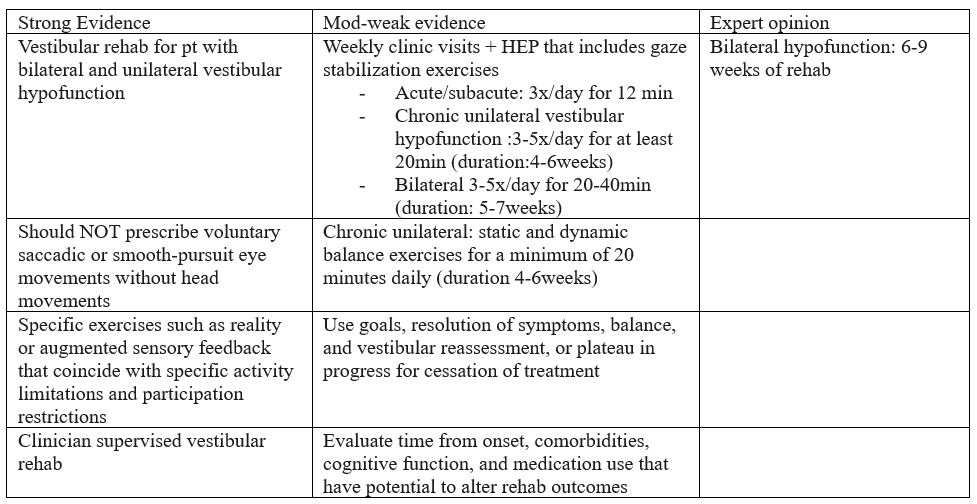
Limitations:
peripheral hypofunction (does not apply to individuals with central disorders)
References:
Hall CD, Herdman SJ, Whitney SL, et al. Vestibular Rehabilitation for Peripheral Vestibular Hypofunction: An Updated Clinical Practice Guideline From the Academy of Neurologic Physical Therapy of the American Physical Therapy Association. J Neurol Phys Ther. 2022;46(2):118-177. doi:10.1097/NPT.0000000000000382
by ptfadmin | Feb 23, 2026 | Health Tips
Reviewed by Tyler Tice, PT, DPT, OCS, ATC
This peer-reviewed article aims to identify the indications, technique, and complications of radiofrequency ablation (RFA). RFA is a minimally invasive procedure that utilizes high-frequency alternating electrical current to generate heat, resulting in targeted tissue destruction. Thermal energy is applied near or on peripheral nerve origins along the spinal cord. Parameters for temperature are designed to spare sensory and motor fibers, targeting only the dorsal root ganglia, which are responsible for transmitting ascending information, such as pain, touch, and temperature.
Indications for this procedure include chronic back and neck pain. Additionally, RFA has been used for radicular pain, discogenic pain, facetogenic pain, post-herpetic neuralgia, post-amputation pain, and post-inguinal herniorrhaphy pain. Contraindications to RFA include patient refusal, increased intracranial pressure, and local infection.
Radio frequency currents are guided via a catheter to an electrode near a nociceptive pathway to intercept pain impulses. The currents heat the surrounding tissue, and the tissue, in turn, heats the electrode. When the target temperature is reached, the current cycles on and off to maintain it.
Potential adverse effects include bleeding, infection, needle placement-induced nerve damage, and burns. Of these, the most common complication is temporary post-procedure discomfort. Other complications may involve alopecia, pigmentation changes (particularly with facial involvement), and neuropathic pain.
The duration of analgesia is dependent on the reinnervation of the targeted tissues by the proximal axons, which typically ranges from weeks to months. In conclusion, RFA should not be used as a stand-alone treatment and is not a substitute for other methods of pain management, but an adjunct treatment.
Reference:
Ray JK, Dixon B, Przkora R. Radiofrequency Ablation. [Updated 2023 Jun 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482387/
by ptfadmin | Feb 19, 2026 | Health Tips
Reviewed by Tyler Tice, PT, DPT, OCS, ATC
This systematic review evaluated the effects of core training on balance in healthy older adults 60 years of age and older. Additionally, the effect of core training on fall prevention was explored. 11 trials were included (RCTs and single-group studies) with 443 older adults from multiple countries. Intervention consisted of core training for a least four weeks. Core training was defined as “traditional core exercise and Pilates-based core programs”.
The focus of core training includes enhancing the stability, coordination, and functional capacity of the abdominals, erector spinae, and iliopsoas. According to this study the effects of core training on older adults has a greater impact on balance and gait performance compared to younger adults likely due to lower balance baseline. Specific exercises and training parameters were not explicitly detailed in the review, making the operational definitions of the interventions unclear.
Balance outcomes were categorized into the following: static, dynamic, or combination. Dynamic balance was defined as the ability to maintain stability while moving through space, regardless of foot movement. Measures used in this study to objectively gauge dynamic balance include Gait Test, Functional Reach Test, and the Timed Get Up and Go. While static balance was defined as the ability to maintain an upright posture with bilateral foot contact on the ground. This was objectively measures using the balance board test and One-Leg Stance Test.
Core training was shown to significantly improve both dynamic and static balance. Sessions greater than 45min yielded greater improvements, most notably on performance of the Timed Get Up and Go. Regarding gait outcomes, traditional core training had more efficacy than Pilates-based training.
Limitations include small number of studies and smaller sample sizes, inconsistent risk for bias across trials, minimal evidence on long-term fall reduction, and heterogeneity in intervention pools.
Overall, the article concluded that core training significantly improves balance, markedly dynamic balance in older adults and it should be integrated into fall-prevention programs. Optimal dosage and long-term effects require further study.
Reference:
Zhong Y, Guo W, Chen P, Wang Y. Effects of core training on balance performance in older adults: a systematic review and meta-analysis. Front Public Health. 2025;13:1661460. doi:10.3389/fpubh.2025.1661460
by ptfadmin | Feb 17, 2026 | Health Tips
Reviewed by John Baur, PT, DPT, OCS, CSCS, FAAOMPT
This talk frames decision‑making as a core coaching skill, not simply a by‑product of collecting more data. French situates modern strength and conditioning (S&C) inside a noisy, high‑velocity information environment where data volume grows faster than human understanding, pressing coaches to develop repeatable processes that translate numbers into training actions. The session’s aim is to help coaches identify, review, and improve strength, power, and conditioning interventions through a structured decision framework. ([NSCA TV][1])
1) The decision environment—complicated vs. complex.
French distinguishes routine, linear problems from complex scenarios characterized by many interacting elements, emergent behavior, and no single “right” answer. In complexity, the coach’s job is to simplify without being simplistic: define the problem space, isolate leading indicators, and stage decisions (e.g., “if this, then that”) so the staff can act decisively under uncertainty. The CEU quiz underscores this by defining *complexity* as “integrated order with too many elements to understand simply,” reinforcing the need for robust but practical heuristics. ([NSCA][2])
2) Time available dictates the mode of thinking.
Decision time is shaped less by the athlete’s mood than by task complexity and the cognitive mode required. When time is short and the setting is familiar, “fast” decisions anchored in practiced rules and thresholds work well; when tasks are novel or stakes are high, the coach deliberately slows the process to an analytical mode. The quiz explicitly flags task complexity and the analytical cognitive mode as the key determinants of how much time a coach needs to decide. ([NSCA][2])
3) The data deluge and bounded rationality.
French cautions that data growth is exponential while understanding is relatively linear, so chasing perfect certainty leads to analysis paralysis. Coaches work under bounded rationality—decisions are limited by the information available and the brain’s capacity to process it. The implication is to pre‑define what “good enough” evidence looks like, protect staff attention, and favor consistent, transparent rules over ad‑hoc judgment. ([NSCA][2])
4) Emotion and human behavior.
French notes that adherence, withdrawal, and performance variability are not purely rational phenomena—emotion sits at the center of human withdrawal behaviors. High‑quality coaching decisions therefore blend objective metrics with interpersonal context and communication strategies that reduce threat and increase athlete buy‑in. ([NSCA][2])
5) From diagnosis to decision: performance determinants > interventions.
When an athlete underperforms (e.g., lower‑body striking is off), the recommended pathway is not to terminate a block or ignore the signal; it’s to identify the performance determinants (strength, rate of force development, tissue tolerance, technical timing, etc.) and adjust the adaptive strategy—volume loading, constraint‑led drills, or recovery emphasis—while monitoring the response. This “determinants‑first” logic is echoed in the quiz. ([NSCA][2])
6) Build a gated profiling pipeline—strength before power.
French describes a gated approach to athlete profiling: first confirm that an athlete meets strength standards relative to their weight class; only then do they “unlock” power profiling. This keeps testing economical, protects time, and prevents advanced diagnostics from obscuring foundational deficits. The talk’s conference listing and quiz both reference this staged approach (strength ➜ power). ([NSCA][3])
7) Force–velocity balance: classify then correct.
Within the power domain, French advocates classifying athletes along the force–velocity spectrum and then programming to pull them toward balance. For a velocity‑dominant profile—what he labels an “antelope”—the corrective emphasis is to train “heavy” to raise force capacity; for a force‑dominant “gorilla,” program on the light/fast side to build velocity. This aligns with NSCA guidance on force–velocity–power profiling as a holistic lens for tailoring training. ([NSCA][2])
8) Programming architecture: general prep starts simple.
In off‑camp general preparation, dynamic strength prescriptions start with a linear loading strategy to establish rhythm, raise chronic workloads safely, and set the stage for later variation (e.g., undulating/wave loading) as camp approaches. This respects the decision principle “simple ➜ complex” and minimizes confounds while the staff is still learning how the athlete responds. The quiz anchors this point with “start with linear loading.” ([NSCA][2])
9) Contact readiness and neck strength ratios.
The session includes neck strength profiling with target flexion:extension ratios to mitigate head/neck risk in contact and collision sports. A commonly referenced target is ~1:1.5–2 (flexion:extension)—recognizing that extensors should be stronger—alongside balanced lateral flexion. Evidence over the past few years supports comprehensive neck training to improve head stabilization and potentially reduce head kinematics during impacts. ([NSCA][2])
10) Turn decisions into a repeatable operating system.
French’s practical message is to codify decision rules—thresholds for advancing from strength to power testing, clear profiles (“antelope” vs. “gorilla”), pre‑planned loading progressions, and communication sequences that account for emotion. This reduces variance between coaches, speeds up choices in complex settings, and keeps the staff focused on interventions that actually change performance, not just dashboards. ([NSCA TV][1])
Overall, the talk urges coaches to think like applied scientists: define the question, choose the smallest valid measure, decide promptly based on bounded evidence, and then observe how the athlete adapts. Iterate quickly, document decisions, and let the athlete’s response—not the prettiness of the graph—drive the next choice. ([NSCA TV][1])
- What does complexity refer to in decision making?
- A simple situation easily understood
- A condition with integrated order and too many elements to understand simply
- A lack of decision‑making structure
Answer: B
- Which factor(s) influences how much decision-making time is required?
- The athlete’s physical condition
- Task complexity and analytical cognitive mode
- The availability of data alone
Answer: B
- What is the main challenge in data growth for modern decision making?
- Data growth is linear and our ability to understand grows exponentially
- Data growth is exponential and understanding is linear
- Data growth matches the capacity to process it
Answer: B
- _________________ is central to human withdrawal behaviors?
- Emotion
- Decision making
- Logic
Answer: A
- What is the impact of “bounded rationality” in decision making?
- Enables unlimited data processing
- Focuses only on rational aspects, ignoring emotions
- Limits decision making to the available information and our ability to process that information
Answer: C
- What decision is recommended for an athlete underperforming on lower body striking?
- Terminate training
- Identify performance determinants and adjust adaptive strategies
- Ignore performance variations until you have more data
Answer: B
- During strength profiling, the athlete is being tested on whether or not they hit performance standards against _________________. If yes, then they unlock the ability to go on to power profiling.
- Weight class norms
- Upper body strength
- Lower body strength
Answer: A
- Dynamic strength prescription during off‑camp general preparation should start with a programming strategy that utilizes a __________________ approach?
- Wave loading
- Linear loading
- Reverse linear loading
Answer: B
- What should the neck flexion to extension strength ratio be for an athlete?
- 1:1
- 1:1.5–2
- 1:3
Answer: B
- What is the recommended approach to balance force and velocity if the athlete is classified as an “antelope?”
- Train on the heavy side to build strength
- Train on the light side to build velocity
- Continue programming as planned; this is a balanced athlete
Answer: A
References
French D. Effective Decision‑Making in Strength and Conditioning
. National Strength and Conditioning Association; 2023. Available at: `https://www.nsca.tv/national-conference/season:7/videos/effective-decision-making-in-strength-and-conditioning` ([NSCA TV][1])
Context on force‑velocity profiling: NSCA. Force‑Velocity‑Power Profile Characteristics. Available at: `https://www.nsca.com/education/articles/kinetic-select/force-velocity-power-profile-characteristics/` ([NSCA][4])
Neck ratio background: Sportsmith. Neck training to improve performance and injury outcomes. Published April 25, 2024. Available at: `https://www.sportsmith.co/articles/neck-training-to-improve-performance-and-injury-outcomes/` ([Sportsmith][5])
[1]: https://www.nsca.tv/national-conference/season%3A7/videos/effective-decision-making-in-strength-and-conditioning “Effective Decision-Making in Strength and Conditioning – 2023 NatCon – NSCA TV”
[2]: https://www.nsca.com/certification/ceu-quizzes/effective-decision-making-in-strength-and-conditioning/ “effective-decision-making-in-strength-and-conditioning | NSCA”
[3]: https://www.nsca.com/globalassets/events/pdf/2023/natcon/nat23-schedule-as-of-7.7.pdf?srsltid=AfmBOoq5NTDbNx-6Rj5cfre4ejQz8dcy6Ld2d3OEimg9Cv8NFlpjpDjN&utm_source=chatgpt.com “2023 National Conference | Las Vegas, NV & Online”
[4]: https://www.nsca.com/education/articles/kinetic-select/force-velocity-power-profile-characteristics/?srsltid=AfmBOop8vVCiPwx3zWKyX1rtWSKFlMFl8KfP4FbkYkNvcjp0qyzvWVub&utm_source=chatgpt.com “Force-Velocity-Power Profile Characteristics”
[5]: https://www.sportsmith.co/articles/neck-training-to-improve-performance-and-injury-outcomes/?utm_source=chatgpt.com “Neck training to improve performance and injury outcomes”
