by ptfadmin | Jun 1, 2026 | Health Tips
Reviewed by: John Baur, PT, DPT, OCS, FAAOMPT
Koc and colleagues present the 2023 revision of the Academy of Orthopaedic Physical Therapy/American Physical Therapy Association clinical practice guideline for heel pain and plantar fasciitis. The article is a focused evidence update intended to help clinicians diagnose, classify, examine, and manage plantar fasciitis within an impairment- and function-based framework. The authors distinguish plantar heel pain as an umbrella term from plantar fasciitis as a more specific clinical entity, emphasizing medial plantar heel pain, tenderness at the medial calcaneal tubercle, and symptoms that are characteristically worse with the first steps after rest or after prolonged weight-bearing.1
The guideline is clinically important because plantar fasciitis is common, often persistent, and frequently seen in both athletic and nonathletic populations. The article notes that plantar fasciitis contributes to approximately 15% of foot pathology in the general population, most often affects adults between 40 and 60 years of age, and may be more common in runners and people whose work requires prolonged standing. Although the term “fasciitis” implies inflammation, the guideline recognizes that the condition may occur along a spectrum that includes inflammatory and degenerative features. This framing is useful because it supports a multimodal plan centered on load management, mobility, tissue tolerance, and function rather than a single inflammatory model.
Methodologically, this revision updates the 2014 clinical practice guideline and concentrates primarily on physical therapist interventions. The authors searched MEDLINE, CINAHL, the Cochrane Library, and PEDro for intervention literature published from December 2012 through March 2023. They graded individual studies by levels of evidence and translated the evidence into recommendation grades ranging from A, reflecting strong evidence, to F, reflecting expert opinion. Risk factors, diagnosis, differential diagnosis, and examination recommendations were largely carried forward from the previous guideline because the authors did not identify new evidence requiring major revisions in those areas. The guideline also explicitly states that it should inform, not replace, individualized clinical judgment and patient preference.
The diagnostic section remains practical and highly usable. Clinicians are encouraged to consider plantar fasciitis when the history and examination show plantar medial heel pain that is most noticeable with initial steps after inactivity, worsens after prolonged weight-bearing, and follows a recent increase in weight-bearing activity. Physical examination findings supporting the diagnosis include pain with palpation of the proximal plantar fascia insertion, a positive windlass test, negative tarsal tunnel tests, limited active and passive talocrural dorsiflexion, abnormal Foot Posture Index-6 findings, and high body mass index in nonathletic individuals. The guideline also highlights risk factors such as limited ankle dorsiflexion, running, and occupational weight-bearing demands, particularly when shock absorption is poor.
The article emphasizes careful differential diagnosis. Clinicians should reconsider the diagnosis or seek consultation when symptoms are inconsistent with plantar fasciitis or fail to improve with appropriate impairment-focused care. Conditions to consider include spondyloarthritis, fat-pad atrophy, proximal plantar fibroma, calcaneal stress fracture, tarsal tunnel syndrome, entrapment of the medial calcaneal nerve or Baxter nerve, S1 radiculopathy, and insertional Achilles tendinopathy. Imaging is usually unnecessary when the clinical presentation is straightforward. If imaging is warranted after failed conservative care or diagnostic uncertainty, the guideline notes that weight-bearing radiographs are generally the first study for chronic foot pain; magnetic resonance imaging without contrast or diagnostic ultrasound may then be considered. Findings such as plantar fascia thickening greater than 4 mm and hypoechoic appearance can support the diagnosis, but imaging abnormalities can be nonspecific and must be interpreted with the clinical picture.
For outcomes and examination, the guideline recommends using validated self-report instruments such as the Foot and Ankle Ability Measure, Foot Health Status Questionnaire, Foot Function Index, and computer-adaptive Lower Extremity Functional Scale. Clinicians should also track reproducible activity limitations and key impairments, including first-step pain, pain with palpation, ankle dorsiflexion range of motion, and body mass index when relevant. The foot and ankle examination outline is broader than a simple heel-pain screen and includes range of motion, joint mobility when deficits are identified, manual muscle testing, heel-raise performance, dorsiflexion lunge testing, Foot Posture Index-6, single-leg squat, gait, balance, special testing, and strategic palpation to assess competing diagnoses.
The strongest intervention recommendations support a multimodal, active, impairment-based plan. Grade A recommendations state that clinicians should use manual therapy directed at lower-extremity joints and soft tissues to address joint and flexibility restrictions, reduce pain, and improve function. Plantar fascia-specific stretching and gastrocnemius/soleus stretching are also strongly recommended for short- and long-term pain reduction and functional improvement. Foot taping, either rigid or elastic, should be used with other physical therapy treatments for short-term improvement in pain and function. Night splints are strongly recommended for a 1- to 3-month period in patients who consistently report first-step morning pain. Importantly, a Grade A negative recommendation states that therapeutic ultrasound should not be used to enhance the benefits of stretching.
Several recommendations are more conditional. Foot orthoses should not be used as an isolated short-term pain-relief treatment, because meta-analyses suggest small to no short-term benefit when orthoses are used alone. However, prefabricated or custom orthoses may be used as part of a combined treatment plan to reduce pain and improve function. Low-level laser therapy has moderate support as part of rehabilitation for short-term pain reduction, while phonophoresis with ketoprofen gel may be used for pain reduction based on weaker evidence. Electrotherapy is positioned as a second-line option; the guideline suggests clinicians may prioritize manual therapy, stretching, and orthoses over electrotherapeutic modalities for short- and long-term outcomes.
The 2023 revision strengthens the role of exercise and dry needling. Clinicians should prescribe therapeutic exercise that includes resistance training for the foot and ankle musculature. Evidence reviewed in the guideline suggests benefit from strengthening programs, heavy-load training, supervised rehabilitation, and multimodal physical therapy that combines education, manual therapy, stretching, resistance training, and neurodynamic interventions. Dry needling to myofascial trigger points in the gastrocnemius, soleus, and plantar foot muscles receives a Grade B recommendation for short- and long-term pain reduction and long-term improvement in function and disability. Reported harms are generally mild, including postneedling soreness and minor bleeding.
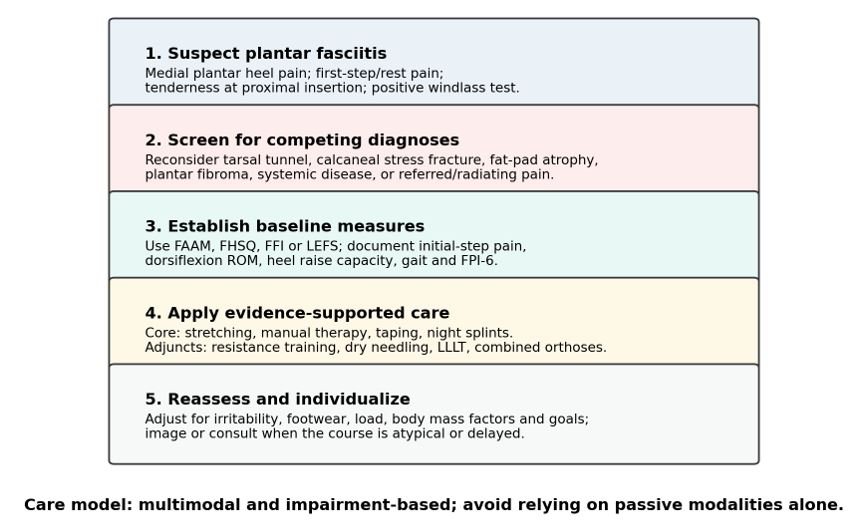
Overall, the guideline provides an actionable framework for clinicians managing plantar fasciitis. Its central message is not that one intervention is universally sufficient, but that care should be matched to patient presentation, irritability, impairments, function, and response over time. High-value care prioritizes stretching, manual therapy, taping, symptom-guided night splints, targeted resistance training, load and footwear counseling, and selected adjuncts when appropriate. The main gaps are not whether treatment can help, but which combinations, doses, and sequencing strategies are most effective for specific subgroups of patients. For clinical practice, the article supports a structured approach: confirm the diagnosis, rule out mimics, measure baseline pain and function, apply evidence-supported interventions, reassess regularly, and escalate or consult when recovery is delayed or atypical.
Visual Synthesis
Figure 1. Evidence strength of major intervention statements. A higher grade reflects stronger supporting evidence, not necessarily a stronger “use” recommendation; some high-grade statements are negative recommendations, such as not using therapeutic ultrasound to enhance stretching.
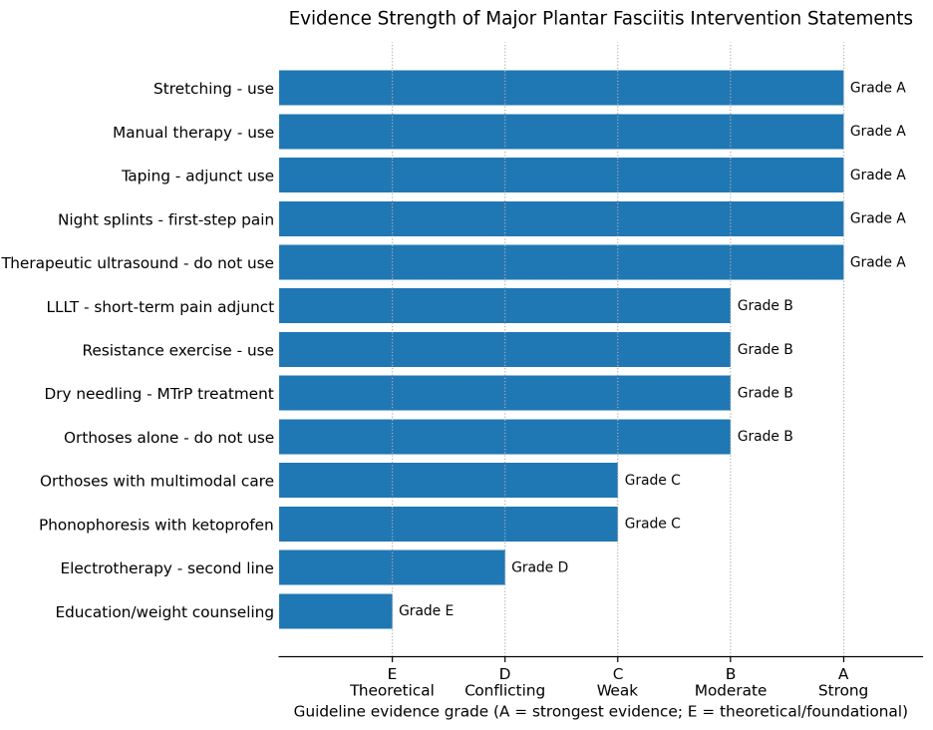
Figure 2. Clinical pathway synthesis derived from the guideline. The figure condenses the article’s decision-making sequence into screening/classification, differential diagnosis, baseline measurement, intervention selection, and reassessment.
Practical Clinical Takeaways
| Clinical Area |
Main Recommendation |
Grade |
Practical Use |
| Diagnosis and screening |
Use clinical pattern recognition: plantar medial heel pain, first-step symptoms, palpation pain at the proximal plantar fascia, positive windlass test, and negative tarsal tunnel testing. |
B |
Rule out mimics when symptoms are atypical or not improving. |
| Core treatments |
Use plantar fascia/gastrocnemius-soleus stretching, manual therapy, taping, and targeted night splints. |
A |
Make these the backbone of conservative care. |
| Orthoses |
Do not use orthoses alone for short-term pain; use prefabricated or custom orthoses only with other treatments. |
B/C |
Most useful as an adjunct when foot posture or taping response supports use. |
| Exercise and loading |
Prescribe resistance training for the foot and ankle musculature. |
B |
Builds local load tolerance and supports long-term self-management. |
| Dry needling |
Use for myofascial trigger points in the gastrocnemius, soleus, and plantar foot muscles. |
B |
Adjunct for pain and disability when clinically indicated. |
| Physical agents |
Avoid ultrasound; LLLT may reduce short-term pain; electrotherapy is second line. |
A/B/D |
Avoid passive modality dominance. |
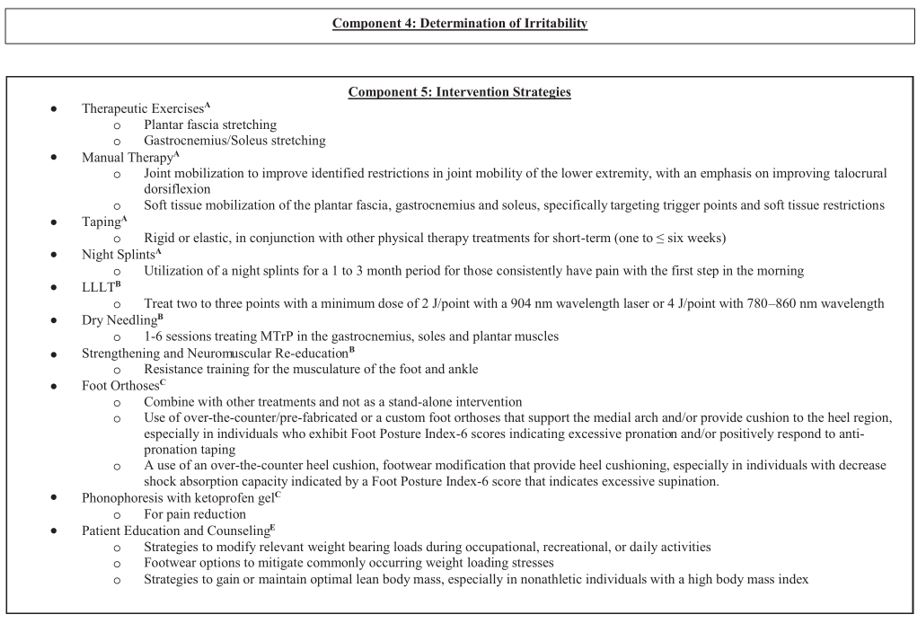
Figure 3. Selected intervention-strategy excerpt from the article’s decision tree (page CPG25). The original guideline states that reproduction and distribution are permitted for educational purposes.
Reference
- Koc TA Jr, Bise CG, Neville C, Carreira D, Martin RL, McDonough CM. Heel pain – plantar fasciitis: revision 2023. J Orthop Sports Phys Ther. 2023;53(12):CPG1-CPG39. doi:10.2519/jospt.2023.0303
by ptfadmin | May 27, 2026 | Health Tips
Reviewed by: John Baur, PT, DPT, OCS, FAAOMPT
Arundale and colleagues present a 2023 clinical practice guideline (CPG) on exercise-based prevention of knee and anterior cruciate ligament (ACL) injuries. The guideline updates the 2018 recommendations from the Academy of Orthopaedic Physical Therapy and the American Academy of Sports Physical Therapy and links prevention strategies to the International Classification of Functioning, Disability and Health. Its central message is practical and direct: athletes, coaches, parents, and clinicians should use structured, exercise-based injury prevention programs to reduce knee and ACL injuries, particularly in young athletes participating in cutting, pivoting, jumping, and field or court sports.1
The scope is intentionally specific. The authors define exercise-based prevention as active movement by the athlete, including strengthening, stretching, neuromuscular training, proprioceptive work, agility drills, plyometrics, and related training. The guideline excludes passive approaches such as bracing and programs that only provide education. It also excludes broad lower-extremity injury programs unless the intervention specifically targeted knee injury outcomes. This focus strengthens the relevance of the recommendations for physical therapists, athletic trainers, strength and conditioning specialists, physicians, coaches, sports scientists, parents, and athletes who are trying to reduce knee injury burden rather than simply improve general fitness.
Methodologically, the CPG is built on a systematic update of the literature published after the prior guideline. With librarian support, the authors searched PubMed, Scopus, SPORTDiscus, CINAHL, and Cochrane databases, first in October 2020 and again in February 2022. Eligible studies included systematic reviews, meta-analyses, randomized controlled trials, cost-effectiveness studies, and higher-level cohort studies. The team used established appraisal tools, including AMSTAR for systematic reviews, PEDro for randomized trials, and the SIGN checklist for cohort studies. Studies below the quality threshold were not used to develop the recommendations. This process supports the guideline’s emphasis on graded recommendations, with Grade A indicating strong evidence, Grade B moderate evidence, and Grade C weaker evidence.
The strongest conclusion is that exercise-based knee injury prevention programs should be recommended for athletes. Across systematic reviews and meta-analyses, such programs reduce overall knee injuries and ACL injuries specifically. A meta-analysis of eight meta-analyses found a 50% reduction in all ACL injuries and a 67% reduction in noncontact ACL injuries among women athletes. Another meta-analysis of eight randomized or cluster-randomized trials including 13,562 participants found a 53% reduction in ACL injury rates among athletes who participated in injury prevention programs. Programs identified as beneficial include 11+ and FIFA 11, HarmoKnee, Knäkontroll, Prevent Injury and Enhance Performance (PEP), Sportsmetrics, and several protocol-specific interventions evaluated in prior trials.1
The guideline gives particular attention to populations with elevated risk or strong evidence of benefit. Women athletes, especially those younger than 18 years, should participate in exercise-based programs before practices, training sessions, or games. Evidence summarized in the CPG indicates that neuromuscular training reduces ACL injury risk in women athletes from approximately 1 in 54 to 1 in 111, with stronger effects in middle school and high school athletes than in collegiate or professional athletes. Soccer players of both sexes are also a priority group. In male collegiate soccer, FIFA 11+ was associated with a lower ACL injury rate, and in elite men’s soccer, specific training modules reduced severe knee injury incidence from 0.68 to 0.38 injuries per 1000 football exposure hours. The guideline also supports prevention programs for team handball athletes, particularly those aged 15 to 17 years.1
Program content matters. The authors emphasize multicomponent neuromuscular training rather than isolated drills. For women athletes, effective programs should include proximal control exercises, strength training, and plyometric exercises. Hip-focused neuromuscular training is highlighted by a prospective intervention in collegiate women’s basketball, where noncontact ACL injuries were reduced after a program that combined education, hip strengthening, balance, and basketball-specific jump-landing exercises. Balance training may be useful, but the CPG states that balance should not be the only program component. The most clinically useful interpretation is that programs should train the athlete to control the trunk, hip, knee, and lower limb during sport-like tasks that involve acceleration, deceleration, cutting, jumping, and landing.1
The guideline also provides implementation details that are often missing from research summaries. Programs should be performed multiple times per week, last more than 20 minutes per session, and accumulate more than 30 minutes per week. They should begin in the preseason and continue through the regular season. High compliance is essential, particularly among women athletes. In practice, this means the program should be scheduled into routine sport participation rather than treated as optional extra work. Many effective programs are designed as dynamic warm-ups before practice or competition, making them easier to integrate without requiring major additional equipment or clinical time.1
A notable recommendation is that prevention should be implemented broadly among young athletes rather than limited to those identified by screening as high risk. The authors argue that universal implementation better mitigates injury and reduces cost, especially among athletes aged 12 to 25 years in sports with high ACL injury risk, including soccer, basketball, rugby, Australian Rules football, netball, and skiing. Programs may be led by coaches, medical professionals, or both. This is important because the success of injury prevention depends less on knowing that programs work and more on whether teams can deliver them consistently across an entire season.1
The CPG is more cautious about secondary prevention after ACL reconstruction. Based on emerging evidence from the ACL-SPORTS trial, clinicians may recommend exercise-based neuromuscular training in the late phase of ACL reconstruction rehabilitation to reduce the risk of future ACL injury. This recommendation is graded as C, reflecting weaker evidence than the primary prevention recommendations. Nonetheless, the finding is clinically important because second ACL injury risk can be substantial in young athletes returning to cutting and pivoting sports.1
The guideline also identifies important evidence gaps. Most research has been conducted in the United States, northern Europe, and Australia, with limited diversity in athlete populations and limited reporting beyond age and sex. More studies are needed in sports beyond soccer and handball, including basketball, volleyball, netball, skiing, and other high-risk sports. The authors also call for research on alternative delivery models, dose-response relationships, strategies to improve adherence, stakeholder engagement, and emerging approaches such as augmented neuromuscular training, biofeedback, and virtual reality. Overall, the article provides a high-value, practice-ready synthesis: exercise-based knee and ACL injury prevention is effective, inexpensive, low risk, and most powerful when delivered early, repeatedly, and consistently as part of normal sport participation.1
Visual Evidence Synthesis
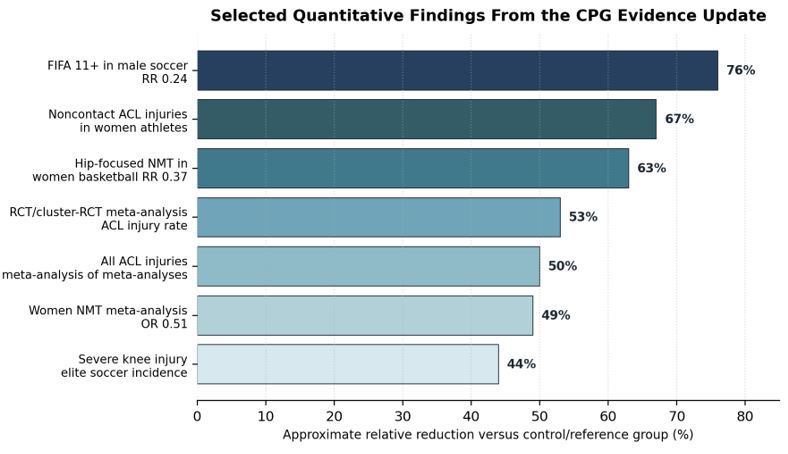
Figure 1. Selected quantitative findings summarized from the guideline evidence update. Percent reductions are orientation estimates derived from reported odds ratios, relative risks, or incidence comparisons and should not be interpreted as directly comparable across populations or study designs.1
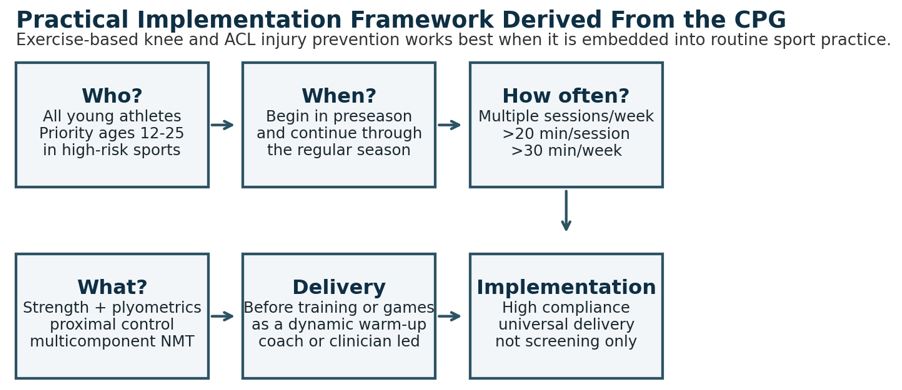
Figure 2. Practical implementation framework derived from the CPG recommendations. The key operational message is to embed neuromuscular training into routine sport participation and monitor compliance throughout the season.1
Key Recommendations and Clinical Interpretation
| Domain |
Guideline Recommendation |
Clinical Interpretation |
| General athlete population |
Recommend exercise-based knee injury prevention programs for prevention of knee and ACL injuries. |
Use validated, structured programs such as 11+/FIFA 11, HarmoKnee, Knäkontroll, PEP, Sportsmetrics, or evidence-based protocol variants. |
| Women athletes and youth |
Implement programs before practices, training sessions, or games, especially in athletes younger than 18 years. |
Prioritize middle school and high school sport settings, where neuromuscular training appears especially protective. |
| Soccer and handball |
Soccer players of both sexes and adolescent handball players should use exercise-based prevention programs. |
Build sport-specific warm-ups into team routines; target jumping, landing, cutting, trunk control, and lower-limb alignment. |
| Program content |
Use multicomponent programs with strength, plyometrics, and proximal control; balance alone is insufficient. |
Train movement quality under sport-like demands rather than relying on isolated static balance exercises. |
| Dose and timing |
Train multiple times per week, longer than 20 minutes per session, and more than 30 minutes per week. |
Start in preseason and continue through the regular season; dose and repetition are central to effectiveness. |
| Implementation strategy |
Implement broadly among all young athletes, not only those screened as high risk. |
Universal delivery can reduce missed cases and improve cost-effectiveness in high-risk sports. |
| Secondary prevention |
Late-phase neuromuscular training after ACL reconstruction may help prevent future ACL injury. |
Useful during return-to-sport preparation, but the evidence is weaker than for primary prevention. |
Table 1. Summary of key clinical practice recommendations and practical implications.1
Reference
- Arundale AJH, Bizzini M, Dix C, et al. Exercise-Based Knee and Anterior Cruciate Ligament Injury Prevention: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability and Health From the Academy of Orthopaedic Physical Therapy and the American Academy of Sports Physical Therapy. J Orthop Sports Phys Ther. 2023;53(1):CPG1-CPG34. doi:10.2519/jospt.2023.0301
by ptfadmin | May 18, 2026 | Health Tips
Reviewed by: John Baur, PT, DPT, OCS, FAAOMPT
Teichert and colleagues conducted a systematic review and meta-analysis to update the evidence on whether exercise interventions prevent new episodes of neck pain in adults without neck pain at baseline. The topic is clinically important because neck pain is common, recurrent, and burdensome in both personal and occupational settings. The article emphasizes that neck pain ranks behind only low back pain among musculoskeletal disorders for years lived with disability, and office workers are a particularly relevant population because annual incidence in that group has been reported as 20% to 50%. Existing clinical practice guidelines have historically focused more on treatment than prevention, leaving uncertainty about whether proactive exercise programs should be implemented before symptoms occur.1
The authors built their review around a focused clinical question: in adults from the general population who were not experiencing neck pain at baseline, do exercise interventions reduce the occurrence of a subsequent neck pain episode compared with no intervention, placebo or sham, attention control, or minimal intervention such as advice or education? Military personnel and astronauts were excluded because their exposure profiles and occupational demands differ substantially from the general population. Eligible interventions included any physical exercise approach judged to be the main part of the intervention. This broad definition allowed inclusion of strength or resistance exercise, stretching, motor control exercise, general physical activity, and combined exercise programs.
The methods were rigorous and reflect contemporary standards for systematic reviews. The authors searched MEDLINE, Embase, CENTRAL, CINAHL, SPORTDiscus, PEDro, ClinicalTrials.gov, and the WHO International Clinical Trials Registry Platform from inception through December 2, 2022. They also performed forward and backward citation searches and contacted authors and experts to identify potentially missed studies. Randomized controlled trials, including cluster randomized trials, were eligible if they followed participants for at least 3 months and reported the occurrence of one or more neck pain episodes. Risk of bias was assessed with the Cochrane RoB 2 tools, and certainty of evidence was judged using the GRADE framework. The meta-analysis used random effects methods, adjusted cluster randomized trials for clustering, and included sensitivity analyses for intracluster correlation assumptions, alternative outcome definitions, adjusted trial estimates, and missing outcome data.
Five trials were included in the meta-analysis. Across these studies, 1,722 participants were randomized at baseline, although the pooled analysis was based on 1,340 participants available at the latest follow-up. The follow-up period ranged from approximately 5 to 12 months. Most participants were office workers, with one study including laboratory technicians; overall, the pooled population was best characterized as workers with primarily static or repetitive occupational demands. The mean participant age was approximately 40 years, and most participants were women. The exercise interventions varied: two trials used resistance programs focused on the neck and shoulder muscles, one trial used stretching combined with motor control exercise, one trial used a walking-based physical activity intervention with financial incentives, and one trial used an individually tailored program in which many participants performed strength and cardiovascular exercise. Comparators were no intervention or minimal intervention, and one trial provided a brief ergonomic assessment to both groups.
The main finding was that exercise interventions probably reduce the risk of a new neck pain episode in the short term, defined as 12 months or less. The pooled odds ratio was 0.49 with a 95% confidence interval of 0.31 to 0.76, indicating that the odds of developing neck pain were about half as high in exercise groups as in control groups. The authors translated this into absolute terms using an assumed 12-month comparator risk of 30%. Under that assumption, approximately 300 of 1,000 people performing mainly static work would be expected to develop neck pain without exercise, compared with about 173 of 1,000 with preventive exercise. This corresponds to 127 fewer cases per 1,000 people, with a number needed to treat of approximately 8 to prevent one episode over 12 months. The absolute benefit changes with baseline risk; at lower baseline risk, the benefit is smaller, while higher-risk populations may experience larger absolute risk reduction.
Despite the favorable pooled estimate, the authors appropriately avoid overstating the findings. The certainty of evidence was rated as moderate, not high, primarily because of study limitations and risk of bias. No trial was judged to be at low overall risk of bias. Two trials had some concerns, and three were rated at high risk of bias, largely because of missing outcome data. The sensitivity analyses for missing data were especially important: when plausible assumptions were made that missing participants in intervention groups may have been more likely to develop neck pain, the confidence interval became compatible with trivial effects. This does not negate the main result, but it lowers confidence in the precision and stability of the effect estimate.
The review has several notable strengths. It updated a prior evidence base that had likely overestimated the preventive effect because of a small number of studies and less robust analytic methods. It included newly published trials, adjusted cluster trials for clustering, used more conservative meta-analytic methods, and provided absolute risk differences that are more clinically interpretable than relative estimates alone. The authors also shared data and statistical code, increasing transparency and reproducibility. These features make the review more trustworthy than earlier summaries of the same question.
The limitations are equally important for clinical interpretation. The body of evidence is small, and most trials were conducted in office or work-related settings, so generalizability to physically demanding occupations, community populations, or people recently recovered from neck pain remains uncertain. Exercise programs were heterogeneous, preventing firm conclusions about the best type, dose, supervision model, or adherence strategy. Outcome definitions varied across trials, and outcomes were self-reported, which is difficult to avoid in prevention studies but still introduces measurement concerns when participants cannot be blinded. The authors also note that harms, costs, health care utilization, sick leave, and productivity were not sufficiently studied, even though those outcomes matter when recommending interventions to people who are currently asymptomatic.
For clinicians, the practical message is that preventive exercise is reasonable to recommend, particularly for office workers and people exposed to prolonged static postures or repetitive computer-based tasks. The findings support the use of exercise as a low-risk preventive strategy, but not as a precisely defined protocol. A pragmatic program might include neck and shoulder strengthening, movement breaks, stretching or motor control work, and general physical activity, selected according to patient preference, work demands, and adherence likelihood. The estimated benefit should be discussed in absolute terms, because patients and employers may judge the value of prevention differently depending on baseline risk, required time, cost, equipment, and tolerance for temporary soreness.
The authors conclude that exercise interventions probably reduce the short-term risk of new neck pain episodes, but whether the range of possible effects is worthwhile should be decided through individualized discussion. Future research should use standardized definitions of a neck pain episode, prospectively registered protocols, better reporting of exercise interventions, careful cluster trial methods, more complete follow-up, and systematic monitoring of adverse events and economic outcomes. Studies should also test strategies to improve adherence and evaluate populations beyond office workers. Overall, the article provides a strong argument for considering exercise-based prevention while maintaining appropriate caution about uncertainty, implementation details, and clinical significance.
Figures and Clinical Interpretation
Figure 1 translates the pooled odds ratio into expected absolute benefit at several plausible baseline risks. Higher baseline risk produces a larger absolute benefit and a lower number needed to treat (NNT).
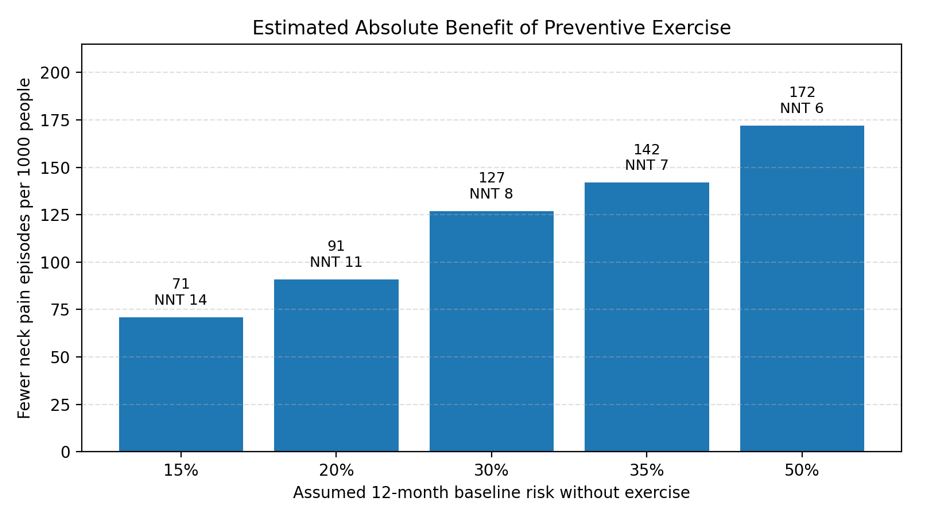
Figure 1. Estimated absolute benefit based on the pooled OR of 0.49 and Table 4 assumptions from the article. NNT = number needed to treat.
Figure 2 reproduces the article’s forest plot of the pooled trial results. The overall effect favors exercise, but the range of trial estimates and the authors’ missing-data sensitivity analyses support cautious interpretation.
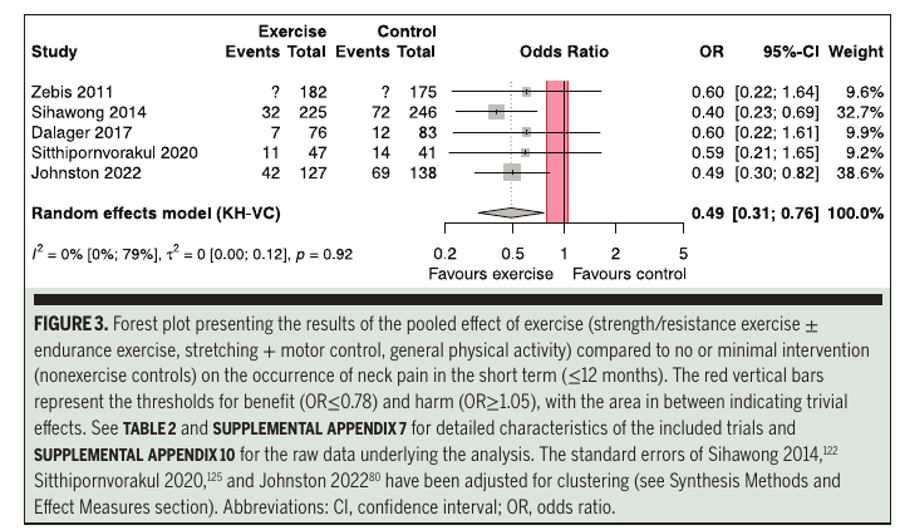
Figure 2. Forest plot of exercise versus no or minimal intervention for short-term neck pain prevention. Reproduced from Teichert et al.
Practical Clinical Takeaways
|
Clinical area
|
Implication
|
Practice note
|
|
Best-supported population
|
Workers with mostly static or repetitive demands, especially office workers.
|
Do not assume the same benefit for all occupations or community populations.
|
|
Intervention choice
|
Evidence supports exercise broadly, not one superior protocol.
|
Use feasible options such as neck/shoulder strengthening, stretching, motor control work, walking, and movement breaks.
|
|
Expected effect
|
At 30% baseline risk, approximately 127 fewer episodes per 1,000 people over 12 months were estimated.
|
Frame benefit in absolute terms; NNT was approximately 8 at this assumed baseline risk.
|
|
Confidence
|
Evidence was moderate certainty and not robust to all missing-data assumptions.
|
Discuss uncertainty and monitor adherence, symptom response, and tolerability.
|
|
Implementation
|
Programs should be easy to perform repeatedly and integrated into daily routines.
|
Workplace programs may benefit from leadership support, reminders, and brief supervised instruction.
|
|
Research gaps
|
Harms, cost-effectiveness, productivity, sick leave, and optimal dose remain uncertain.
|
Future trials should use standardized episode definitions and better follow-up.
|
Reference:
- Teichert F, Karner V, Döding R, Saueressig T, Owen PJ, Belavy DL. Effectiveness of exercise interventions for preventing neck pain: a systematic review with meta-analysis of randomized controlled trials. J Orthop Sports Phys Ther. 2023;53(10):594-609. doi:10.2519/jospt.2023.12063
by ptfadmin | May 11, 2026 | Health Tips
Reviewed by: John Baur, PT, DPT, OCS, FAAOMPT
Chimenti and colleagues present the 2024 revision of the Academy of Orthopaedic Physical Therapy clinical practice guideline for Achilles pain, stiffness, and muscle power deficits related specifically to midportion Achilles tendinopathy. The guideline is intended for physical therapists and other clinicians who manage posterior ankle pain and tendon-related functional limitations.1 It updates prior 2010 and 2018 guidance by incorporating literature published through March 7, 2024, with particular emphasis on physical therapy interventions. The authors define tendinopathy as local tendon pain associated with tendon-loading activities, which is important because the term avoids assuming that inflammation or degeneration is the sole cause. The scope is deliberately narrow: it addresses midportion Achilles tendinopathy, typically pain located more than 2 cm proximal to the calcaneal insertion, and does not directly generalize to insertional Achilles tendinopathy.
The guideline frames midportion Achilles tendinopathy as a common, functionally limiting overuse condition affecting athletic and nonathletic populations. The article notes a reported prevalence of approximately 4% to 7%, with higher prevalence associated with increasing age and greater athletic involvement. Runners are highlighted as a particularly relevant population, with prior data suggesting a substantial lifetime chance of Achilles tendon injury. The clinical course is variable. Most individuals improve, but recovery may take months and depends on a combination of biological, functional, psychosocial, and disability-related factors. The authors emphasize that symptom duration alone may not be a strong predictor of response; acute and chronic presentations can both improve with appropriate tendon-loading rehabilitation. Symptom irritability, load tolerance, lower extremity strength and endurance, body mass index, tendon morphology, fear of movement, pain beliefs, and self-efficacy may all influence progress.
Diagnosis remains primarily clinical. The 2024 summary recommends identifying symptoms localized to the Achilles tendon midportion, pain provoked by tendon-loading activities, pain with palpation of the tendon midportion, and tendon thickening when present. The Royal London Hospital test and painful arc sign remain useful examination findings, although localized thickening can be absent in some patients. The guideline also highlights differential diagnosis. Clinicians should reconsider the diagnosis when symptoms do not fit the expected pattern or do not improve with appropriate rehabilitation. Important alternatives include partial Achilles tendon tear, retrocalcaneal or subcutaneous bursitis, posterior ankle impingement, sural nerve irritation, tibial or calcaneal stress fracture, os trigonum syndrome, accessory soleus muscle, Achilles tendon ossification, systemic inflammatory disease, plantaris involvement, paratenonitis, fascial tears, and insertional Achilles tendinopathy.
The article takes a selective approach to imaging. Ultrasound, radiographs, and magnetic resonance imaging can support clinical reasoning when the diagnosis is uncertain, recovery is delayed, symptoms worsen during care, or an invasive procedure is being considered. Imaging is not required for routine diagnosis, and the authors caution that structural findings must be interpreted in context. Increased tendon thickness, for example, is common in symptomatic tendinopathy but can also appear in asymptomatic adults. Ultrasound is presented as accessible, low cost, and useful for visualizing soft tissue, while radiographs help assess bony contributors and MRI is generally reserved for specific diagnostic or procedural planning needs.
The strongest recommendation is for tendon-loading exercise as first-line care. Clinicians should use loading exercises, at the highest load tolerated, to decrease pain and improve function in individuals without presumed tendon-structure frailty. This recommendation is not limited to eccentric training. The CPG uses the broader term tendon loading to include eccentric, concentric, isometric, isotonic, heavy slow resistance, and plyometric loading of the plantar flexors. Evidence summarized in the article indicates that exercise improves pain and function compared with wait-and-see or passive approaches, with clinically meaningful improvements appearing as early as two weeks and commonly reaching approximately 18 to 21 points on the Victorian Institute of Sports Assessment-Achilles scale by 12 weeks. The guideline advises exercise at least three times weekly at an intensity as high as tolerated, while recognizing that clinicians must adjust volume and intensity based on irritability, functional capacity, and total daily tendon load.
Education and counseling are the second core intervention. The authors recommend combining tendon loading with either pain science education or pathoanatomic education. Both approaches can be effective, and delivery may occur in person, by telehealth, or through a hybrid model depending on the patient’s preference. A key message is that complete rest is not indicated. Patients should continue activity within pain tolerance, using symptoms to guide progression rather than avoiding tendon loading entirely. This point is central to the clinical logic of the guideline: recovery is built around graded exposure, confidence, and restoration of load capacity rather than passive protection alone.
Several adjunct interventions may be used selectively, but none replace exercise and education. Stretching may be used when ankle dorsiflexion restriction is present. Neuromuscular re-education may target lower extremity movement impairments that contribute to abnormal Achilles loading. Manual therapy may be applied to muscles, joints, or connective tissues when mobility deficits are present, although the recommendation is based on expert opinion rather than strong clinical trial evidence. Intramuscular dry needling may be considered for calf-related pain and stiffness, especially in more acute cases or when patients cannot yet tolerate progressive loading. Heel lifts may temporarily reduce dorsiflexion demands during activity. Taping may be used to reduce pain, alter foot posture, or reduce tendon strain, but supporting evidence is largely theoretical or indirect. Orthoses remain an area of uncertainty because evidence is contradictory.
The guideline is also explicit about interventions that should not be emphasized. Low-level laser therapy should not be used for midportion Achilles tendinopathy, and therapeutic ultrasound should not be used as a stand-alone treatment. Night splints remain unsupported for improving symptoms. Multimodal treatment may be used to enhance exercise effects, but the article stresses that the best combination of adjuncts is unclear, and many network meta-analysis rankings are limited by small samples, heterogeneity, and risk of bias. Overall, the CPG discourages passive modality-driven care and encourages impairment-based, active rehabilitation.
Outcome measurement is another strength of the article. Clinicians are advised to track patient-reported symptom severity and activity limitations using tools such as the VISA-A, Foot and Ankle Ability Measure, or Lower Extremity Functional Scale. The CPG also points to newer Achilles-specific measures, including the TENDINopathy Severity assessment-Achilles and VISA-A sedentary, which may be useful in nonathletic populations. Physical performance measures such as heel-rise endurance, hop testing, movement-evoked pain during loading, ankle range of motion, plantar flexor strength and endurance, gait, and palpation findings help clinicians document baseline impairment and response to treatment.
The decision tree on pages 18 and 19 translates these recommendations into a practical workflow. It begins with medical screening, proceeds through diagnosis and differential evaluation, then classifies patients by symptom irritability and load tolerance. Patients with low load tolerance may require lower-load tendon exercise, temporary unloading strategies, mobility interventions, and careful symptom monitoring before progressing. Patients with higher load tolerance can generally begin higher-intensity mechanical loading sooner. The guideline’s definition of successful recovery at 6 to 12 months includes a VISA-A score greater than 80, tolerable intermittent pain, resumed primary activities, and achievement of patient goals. If progress is poor, the pathway recommends re-evaluation and referral when needed.
Overall, this 2024 CPG supports a patient-centered, active, and load-progressive approach to midportion Achilles tendinopathy. Its most actionable message is that tendon-loading exercise and education form the foundation of care, while adjuncts should be selected only when they address a specific impairment, symptom barrier, or activity need. The article is methodologically transparent, uses formal evidence grading, and clearly separates strong recommendations from weak, conflicting, theoretical, or expert-opinion guidance. Its main limitations are the incomplete evidence base for acute presentations, sedentary patients, psychosocial subgroups, exercise dose selection, and many adjunct interventions. Nevertheless, the guideline gives clinicians a clear framework: diagnose clinically, avoid unnecessary imaging, keep patients active within tolerance, progressively rebuild tendon capacity, monitor meaningful outcomes, and reserve passive or invasive pathways for situations in which active rehabilitation does not produce adequate improvement.
Visual Synthesis
Figure 1. Distribution of recommendation strength across the article’s 2024 intervention recommendations.
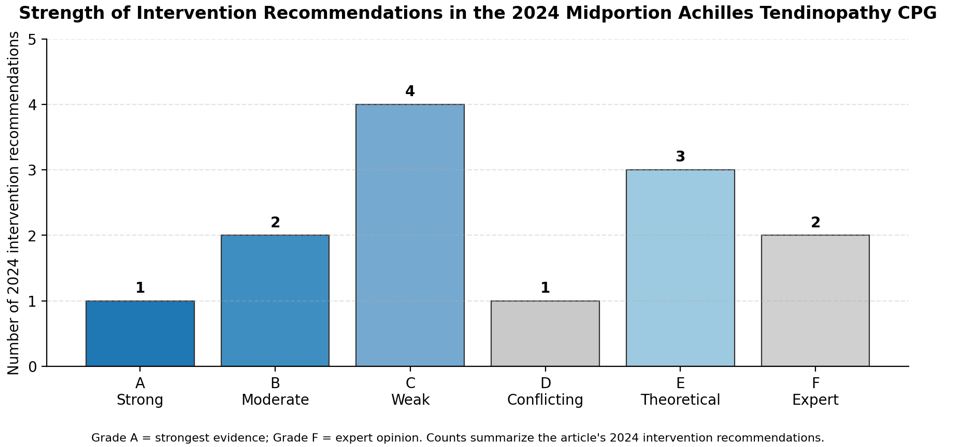
The chart shows that only tendon-loading exercise receives a Grade A recommendation, while several adjunctive strategies remain weak, theoretical, conflicting, or expert-opinion based.
Figure 2. Simplified management pathway based on the guideline decision tree and intervention recommendations.
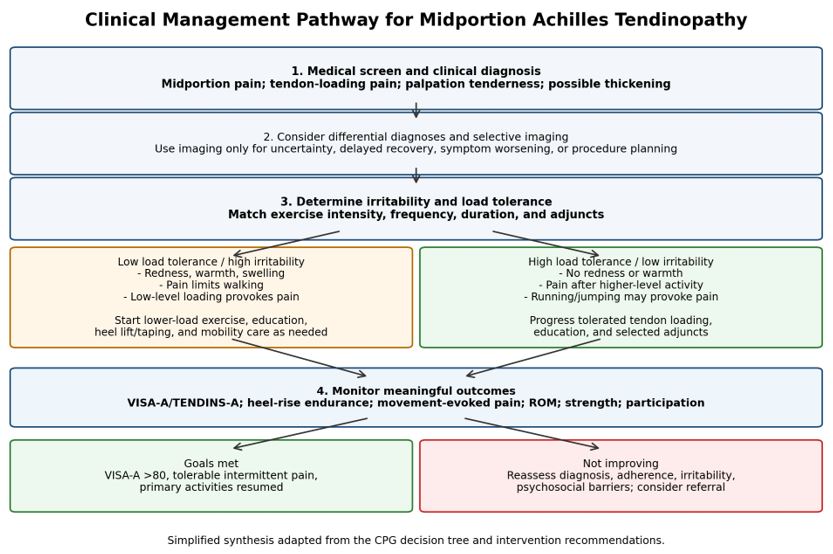
This pathway summarizes the article’s sequence of screening, clinical diagnosis, differential diagnosis, irritability staging, intervention matching, outcome monitoring, and referral or discharge decision-making.
Practical Clinical Takeaways
|
Care Element
|
Guideline Direction
|
Clinical Implication
|
|
Tendon-loading exercise
|
Grade A first-line treatment; exercise at least 3 times weekly at high tolerated intensity.
|
Build load capacity using eccentric, concentric, isometric, isotonic, heavy slow resistance, and/or plyometric progressions.
|
|
Education and activity
|
Grade B recommendation to combine education with exercise and avoid complete rest.
|
Use pain monitoring, graded exposure, reassurance, and shared decision-making to keep patients active within tolerance.
|
|
Adjunctive mobility or symptom tools
|
Manual therapy and dry needling may be used selectively; heel lifts and taping may provide temporary offloading or symptom relief.
|
Use adjuncts to address defined impairments or barriers, not as substitutes for progressive loading.
|
|
Passive modalities
|
Low-level laser should not be used; therapeutic ultrasound should not be used alone; night splints remain unsupported.
|
Prioritize active rehabilitation and avoid treatment plans centered on low-value passive modalities.
|
|
Monitoring and escalation
|
Use patient-reported outcomes and performance measures; re-evaluate when recovery is delayed.
|
Track VISA-A/TENDINS-A, heel-rise endurance, movement-evoked pain, ROM, strength, and return-to-activity goals; refer when indicated.
|
Note. Recommendation grades reflect the article’s evidence hierarchy: A = strong evidence, B = moderate evidence, C = weak evidence, D = conflicting evidence, E = theoretical/foundational evidence, and F = expert opinion.
Reference
Chimenti RL, Neville C, Houck J, Cuddeford T, Carreira D, Martin RL. Achilles pain, stiffness, and muscle power deficits: midportion Achilles tendinopathy revision – 2024: clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health from the Academy of Orthopaedic Physical Therapy of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2024;54(12):CPG1-CPG32. Published online November 27, 2024. doi:10.2519/jospt.2024.0302
by ptfadmin | Apr 21, 2026 | Health Tips
By Hannah E. Cabre
Reviewed by; John Baur, PT, DPT, OCS, FAAOMPT
Cabre’s narrative review examines how nutrition guidance for strength and conditioning athletes should be adapted for adult, premenopausal cisgender female athletes. The central argument is that sports nutrition practice has advanced faster than the female-specific evidence base. Although women now make up a large share of collegiate sport participation, many calorie, carbohydrate, protein, fat, and supplement recommendations are still extrapolated from studies in men. The review warns that this gap encourages oversimplified advice, including social-media “cycle syncing” claims, and may contribute to inconsistent fueling recommendations that place female athletes at risk for inadequate intake.1
The article first explains that women respond strongly to resistance training. Absolute strength gains are often lower than men’s because of differences in muscle mass and contractile properties, but relative improvements in strength and hypertrophy can be similar, and in some studies greater, in women. Physiologically, women generally have more type I fibers, greater oxidative capacity, better fatigue resistance, and greater reliance on fat oxidation than men, whereas men tend to have greater glycolytic capacity. Estrogen and progesterone fluctuate across the menstrual cycle and can alter substrate use, energy expenditure, recovery, and fluid balance. However, recent evidence suggests that resistance-exercise-stimulated muscle protein synthesis is not meaningfully changed by menstrual cycle phase, so phase-based protein strategies are not supported.
Energy availability is presented as the foundation of health and performance. The review emphasizes Relative Energy Deficiency in Sport (REDs), defined as a mismatch between energy intake and exercise expenditure that can impair metabolism, reproductive function, bone, immune, cardiovascular, and musculoskeletal health. Low energy availability in women is identified as less than 30 kcal per kilogram of fat-free mass per day, while approximately 45 kcal/kg fat-free mass/day is suggested to avoid low energy availability. The author notes that estimating calories for resistance training is difficult because anaerobic work is hard to capture, wearable devices are often inaccurate, and predictive equations should match the athlete’s age, body size, activity level, and life stage. Pregnancy and lactation require special attention because energy and nutrient demands increase, and training may need modification.
For carbohydrates, the review balances performance needs with female-specific metabolism. Carbohydrate remains the primary fuel for high-intensity activity, yet female strength athletes may use less muscle glycogen during resistance exercise than men. Therefore, carbohydrate loading is not automatically necessary. A practical range of 3-7 g/kg/day is recommended depending on training volume, intensity, and daily activity, with 30-60 g/hour during sessions if fatigue limits performance. Carbohydrate supplements can help when food intake is insufficient, but they should not crowd out protein.
Dietary fat is framed as essential for energy density, hormonal function, inflammation control, and recovery. Because women rely more heavily on fat metabolism, adequate fat may be especially important in strength and conditioning contexts. The review recommends at least 15%, and ideally about 20%, of total calories from fat, with approximately 1 g/kg/day during weight maintenance and lower ranges only when supervised fat loss is appropriate. Unsaturated fats and omega-3 intake are emphasized, while trans fats and excessive saturated fats should be limited.
Protein guidance is similar to male athlete recommendations because available evidence suggests comparable protein turnover and muscle protein synthesis responses. Female strength athletes should consume at least 1.5 g/kg/day, within the broader 1.4-2.0 g/kg/day sports nutrition range. The article highlights the value of distributing high-quality protein across the day, targeting essential amino acids and roughly 2.5 g leucine per serving, and consuming 0.32-0.38 g/kg before and after resistance training. A small pre-sleep protein serving may reduce overnight breakdown.
The supplement section focuses on caffeine, creatine monohydrate, and protein powders. Caffeine may support aerobic and anaerobic performance at 3-6 mg/kg about 60 minutes before exercise, although menstrual cycle and contraceptive effects require more study. Creatine is presented as well supported and potentially valuable for women, improving high-intensity power, fatigue measures, cognition, mood, and luteal-phase fluid balance without clear evidence of phase-related weight gain. Protein powders can help meet daily needs when whole foods are limited, especially whey or casein sources rich in leucine.
Overall, the article calls for evidence-based, individualized practice rather than rigid sex stereotypes. Coaches, dietitians, and health practitioners should monitor energy availability, menstrual and pregnancy-related changes, training demands, hunger, fatigue, and recovery. The review’s limitation is the limited female-specific evidence, including small samples, inconsistent menstrual-cycle tracking, and underrepresentation of elite athletes. Its practical contribution is a cautious framework that supports performance while prioritizing long-term health.1
Reference
- Cabre HE. Optimizing performance and health: nutrition considerations for female athletes in strength and conditioning. Strength Cond J. 2025;47(6):619-629.
by ptfadmin | Mar 23, 2026 | Health Tips
Reviewed by Tyler Tice, PT, DPT, OCS, ATC
This scoping review published in Sports Medicine (2024) synthesized literature from 1986–2023, including both published and unpublished studies, to examine the influence of menstrual cycle phases (MCP), menstrual irregularities (MI), and hormonal contraceptive (HC) use on musculoskeletal (MSK) injuries among female athletes aged 13–45 years. The study designs included are as follows: cross-sectional (43), cohort (21), case-control (12), case series (11), case studies (7), and randomized controlled trials (1)
Most studies investigated menstrual irregularities and menstrual cycle phases as injury risk factors. Additionally, most of the research focused on elite or professional-level athletes. Pregnant, perimenopausal, and menopausal women were excluded.
Hormonal Influence on Injury Risk
Injury rates in comparable sports are generally higher among female athletes. Continuous hormonal fluctuations are hypothesized to influence the structure and mechanical properties of muscle, tendon, bone, and ligaments. Both menstrual function and hormonal contraceptive use alter endogenous reproductive hormone levels, potentially affecting injury risk. A typical menstrual cycle includes the follicular phase, ovulation, and the luteal phase respectively. Hormonal fluctuations throughout these phases have been associated with increased risk of both acute and overuse injuries.
In female soccer players, injury incidence appears greatest during the late follicular phase. Increased risk of muscle, tendon, and anterior cruciate ligament (ACL) injuries has also been observed during this phase. Additionally, peak estrogen levels during ovulation are associated with increased ligament laxity, altered strength, and reduced neuromuscular control, which may predispose athletes to injury. However, findings across studies are inconsistent, and a direct causal relationship between menstrual cycle phase and injury has not been definitively established.
Menstrual Irregularities and Injury
Menstrual irregularities are prevalent among female athletes and are associated with elevated injury risk. High school athletes with menstrual dysfunction demonstrate greater time-loss severity compared to athletes with regular menstrual cycles.
The Female Athlete Triad, now referred to as Relative Energy Deficiency in Sport (RED-S), highlights the interrelationship between low energy availability, menstrual dysfunction, and reduced bone mineral density. RED-S also has implications for cardiovascular health, immunity, metabolic rate, and overall menstrual function. Athletes with menstrual irregularities are particularly susceptible to bone stress injuries due to reduced estrogen levels and compromised bone health.
Hormonal Contraceptives and Injury Risk
Approximately half of female athletes use hormonal contraceptives, including: oral contraceptive pills (OCPs), intrauterine devices (IUDs), injections, transdermal patches, implants, and vaginal rings. Hormonal contraceptives suppress endogenous hormone production and eliminate typical cyclical fluctuations. Some literature included in this review suggests that hormonal contraceptives, particularly oral contraceptives, may provide a protective effect against injury. Among female athletes, some studies suggest that oral contraceptive use, with or without neuromuscular training, may improve dynamic knee stability and potentially reduce ACL injury risk. However, evidence from the general population indicates that combined hormonal contraceptives are not protective against MSK injuries.
Overall, evidence remains inconclusive due to methodological variability across studies. Despite inconsistencies in the literature, physical therapists should not dismiss menstrual and hormonal influences, as they may represent an important piece of the multifactorial puzzle in injury risk and rehabilitation for female athletes.
Reference:
MacMillan, C., Olivier, B., Viljoen, C. et al. The Association Between Menstrual Cycle Phase, Menstrual Irregularities, Contraceptive Use and Musculoskeletal Injury Among Female Athletes: A Scoping Review. Sports Med 54, 2515–2530 (2024). https://doi.org/10.1007/s40279-024-02074-5
Page 2 of 49«12345...102030...»Last »