by ptfadmin | Apr 3, 2024 | Health Tips
Reviewed by: Zachary Stango, SPT; Bridget Collier, PT, DPT
The increase in virtual reality and gamification has been implemented in numerous aspects of our daily lives, and the area of rehab is one realm in which advancements in technology have the possibility to make tremendous impacts on patient outcomes. The randomized controlled trial conducted by Afzal et al. (2022) aimed to analyze the effects of implementing virtual reality exercises into a physical therapy routine, on pain and perceived disability, in patients with chronic low back pain.
The inclusion criteria for this study consisted of participants aged 25-50 with a history of chronic low back pain, which the study defined as pain persisting for greater than 12 weeks. Patients were randomly assigned to a group receiving conventional physical therapy, consisting of a moist heat pack, hamstring stretching, and loading and stretching of the lumbar spine musculature. The experimental group underwent the same therapeutic interventions, with the addition of two virtual reality interventions: the reflex ridge and body ball game. The reflex ridge made participants complete movements such as trunk side bending, sitting, and jumping to avoid obstacles on the screen. The body ball game included arm movements while kicking a ball displayed on the device. Each group underwent their respective interventions three times a week for a total of 12 weeks, with metrics analyzed after every quarter completion of the study. The 84 participants had their pain levels measured using the Visual Analogue Scale (VAS) and their perceived disability measured through the Modified Oswestry Disability Index (MODI). Both of the groups displayed significant improvements in their levels of pain and subjective disability, with the group undergoing the additional virtual reality interventions exhibited significant reductions in their scores compared to the conventional group, correlating with better outcomes.
Clinical Bottom Line:
Virtual reality allows for the participants to dive into their own world of adventure, and the rehabilitative world can use this tool to allow patients the opportunity to actively complete tasks in their animated realm, which could translate to completion of these tasks in everyday life. Even though the activities in this study that were completed in virtual reality did not necessarily mimic activities of daily living for every participant, the motions can serve as a starting point to progress these to add in loading of the lower back. Individuals with chronic low back pain often show signs of fear avoidance of specific movements and the results of this study suggest that virtual reality can aid in helping these individuals regain the confidence to complete previously avoided movements and return to their prior level of function.
References:
Afzal MW, Ahmad A, Mohseni Bandpei MA, Gilani SA, Hanif A, Waqas MS. Effects of virtual reality exercises and routine physical therapy on pain intensity and functional disability in patients with chronic low back pain. J Pak Med Assoc. 2022;72(3):413-417. doi:10.47391/JPMA.3424
by ptfadmin | Mar 27, 2024 | Health Tips
Reviewed by Tyler Tice, PT, DPT, OCS, ATC
Introduction:
Neuromuscular disorders that result in the demyelination of neurons, like multiple sclerosis (MS), experience several motor, sensory, and cognitive deficits over the disease’s progression. Reduction in balance capabilities is common among this population and is a major reason for these patients to seek out physical therapists to combat the degeneration that occurs over time. It is well understood and recommended that all older adults with chronic health conditions like MS participate in moderate to high-intensity balance training at least 2-3 times per week to avoid increasing their risk of falls. This review looked to synthesize how training frequency, intensity, time components, duration, and progression in balance training can be best completed for people living with MS.
Methods:
This review included 40 eligible studies which had to be of randomized control/clinical trial or systematic review in origin. Inclusion criteria required all participants to be adults with a diagnosis of MS, a severity level of 7.5 or lower on the Expanded Disability Status Scale, be able to transfer from one seated position to another independently, and at least 50% of exercise interventions used in the trials must have been directly relate to challenging balance control.
Conclusions of the Study:
This study effectively synthesized the major components of designing a balance training program. The majority of the exercises performed challenged general motor and sensory deficits commonly seen in MS, but fewer studies included training of reactive motor strategies, and even less challenged tasks requiring cognitive dual tasking. This aspect was surprising as cognitive dual-tasking ability is a strong indicator of potential fall risk for patients with MS. The balance training progression among each of the studies also had no specific method and seemed to be specific to the clinician treating the patient. The researchers stated that the exact order in which progression is made does not matter whether that is through changing the base of support, the cognitive demand of the task, or the somatosensory deficit being targeted as long as the task is challenging the patient’s specific deficits. Balance training intensity also had no common system among any of the studies and was oddly not measured often. Two studies utilized visual displacement of the center of mass and the excessive corrective upper limb movements as indicators of failure of an exercise, while others cited the patient’s perception of difficulty as their marker for intensity. The researchers concluded that there is a current lack of evidence providing clinicians with specific parameters to program and progress their patients and that future research should be performed to determine better guidelines for treating MS patients.
Clinical Implications:
Based on this review, the current state of evidence on exercise programming specifics for balance training in patients living with MS is mostly inconclusive. The best method of proceeding with treating individuals with MS would be to first identify what systems have been affected most by the MS, whether it is more motor, sensory, or cognitive. The second step would be to determine your progression model based on how the patient presents and their goals. For example, deciding when to incorporate cognitive dual tasks or to reduce the patient’s base of support first. Furthermore, when gauging the intensity of balance exercise it is recommended to determine the patient’s perception of intensity, such as with an RPE scale, and to also gauge the patient’s difficulty through observing the visual displacement of the patient’s center of mass and any excessive corrective upper limb movement. Combining the use of both these factors should improve the reliability of determining the patient’s exercise intensity. By taking these components into account a PT should be able to effectively program and progress a patient’s balance training program and tailor it to their goals.
References:
Brincks, J., Dalgas, U., Franzén, E., Callesen, J., Wallin, A., & Johansson, S. (2023). Unwrapping the “Black Box” of balance training in people with multiple sclerosis – a descriptive systematic review of intervention components, progression, and intensity. Multiple Sclerosis and Related Disorders, 69, 104412. https://doi.org/10.1016/j.msard.2022.104412
by ptfadmin | Mar 20, 2024 | Health Tips
Reviewed by Tyler Tice, PT, DPT, OCS, ATC
Introduction:
Cervicogenic headaches are a common form of headache that impacts up to 20% of the population. These headaches commonly come from the musculoskeletal components surrounding the cervical spine and are exacerbated by neck movements. Current clinical practice guidelines suggest manual technique usage in conjunction with exercise as the best course of treatment, with some of the most common manual techniques utilized being mobilizations and manipulations. This study intended to determine which method is more effective in reducing patient discomfort and improving function in patients who have cervicogenic headaches.
Methods:
The study was a randomized pragmatic clinical trial that required all patients to be diagnosed with cervicogenic headaches, have tenderness to palpation in at least one joint in the upper cervical spine region, a neck disability index (NDI) of at least 20% or greater, and at least a 2/10 level of pain on the NPRS pain scale. All patients completed several self-report measures including the NDI, Headache impact test, and NPRS pain scale. The study compared upper cervical spine (C0-C3) mobilizations versus manipulations of the same area.
Conclusions of the Study:
The study concluded there was no difference in the patient’s perceived improvements in pain and function and objective ROM. This contradicts previous evidence stating that manipulations provided greater improvements in patient-reported outcomes than mobilizations. However, many previous studies utilized a prescriptive approach that had all manipulations and mobilizations performed at the same location, whereas this study utilized a pragmatic approach that allowed the treating therapists to use their own clinical judgment to determine where to perform manual techniques. It can be concluded from this study that despite there being some limitations, especially the smaller sample size of 45 people, that when treating patients with cervicogenic headaches both manipulations and mobilizations are viable options to improve patient pain and disability.
Clinical Implications:
This study provides some evidence for the idea that manipulation or mobilization for cervicogenic headache patients can have nearly the same effect on patient perceived functionality. Given the increased risks of performing upper cervical spine manipulations it may be better to defer to mobilizations when deciding on manual treatments for patients with cervicogenic headaches, unless mobilizations have otherwise been unsuccessful. The similar improvements seen may be due to the neurophysiological input to the brain that is improving patient functionality, rather than any increases in motion after mobilization or manipulation. The key part of this study that differs from previous research is its allowance of the PT’s clinical judgment to determine what the patient needs during treatment. This highlights the importance of reassessing from session to session to determine exactly what the patient may benefit from more, it is important to keep in mind the differences in the methods of this study compared to previous iterations.
Reference
Lerner-Lentz, A., O’Halloran, B., Donaldson, M., & Cleland, J. A. (2020). Pragmatic application of manipulation versus mobilization to the upper segments of the cervical spine plus exercise for treatment of cervicogenic headache: A randomized clinical trial. Journal of Manual & Manipulative Therapy, 29(5), 267–275. https://doi.org/10.1080/10669817.2020.1834322
by ptfadmin | Mar 15, 2024 | Health Tips
Reviewed by Tyler Tice, PT, DPT, OCS, ATC
Introduction:
Shoulder pain is incredibly common among the general population with a prevalence of between 7-26%. Most of this shoulder pain is attributed to the generalized term of Subacromial pain syndrome (SAPS), subacromial impingement syndrome, rotator cuff tendinopathy, or some other variant of these. This dysfunction is traditionally linked to overuse or dysfunction of underlying structures in the area of glenohumeral joint, altered kinematics of the shoulder, or slouched posture. This meta-analysis looks to compare patient treatment outcomes when they take part in an intensive supervised exercise program, a home training program, and no training at all.
Methods:
The systematic review included studies with populations of non-traumatic event related shoulder pain with pain lasting at least 1 month before seeking professional help and no other clear diagnosis at hand. Supervised training was defined as training instructed by a healthcare professional two or more times. Home Training included a take home leaflet from a healthcare professional or one time instruction, but no other instruction, and no training received was no instruction at all and were left to heal without therapy. The study lengths ranged from being 6 weeks to 6 months long and used multiple patient reporting handouts to determine patient pain and functionality.
Conclusions of the Study:
The review determined that having supervised training was better than no training at all and improved pain at rest and during movement, shoulder function, and patient perceived effect. However, supervised training and home training had equal effects on pain and shoulder function. The researchers stated that supervised training saw greater benefits in patients with higher pain levels and disability levels at baseline, as well as greater adherence to the training protocol. This suggests that the clinician will have to use their clinical judgement to determine which patients will benefit from more of a home based exercise program, and which will require more in person supervision to recover from SAPS or other similar conditions.
Clinical Implications:
This paper gives insight to the necessity of a PT’s judgement when treating their patient’s. The improvements in pain and shoulder function patient’s receive from exercise can be seen regardless of whether it is supervised for multiple visits per week within clinic or unsupervised at home. The key is to take into account the patient’s stage of healing, irritability levels, baseline level of function, and attitude toward exercise to decide if they can make progress on their own. If the patient happens to be in a high irritability state incorporating several sessions of supervised therapy may be greatly beneficial to build the patient’s confidence and comfort with performing exercises on their own, in conjunction with manual techniques to desensitize the painful areas. This may allow the therapist to eventually transition the patient to a self-management home exercise program. The goal should be to educate and empower patients to understand the benefits of the exercise and be able to manage their own rehabilitation at home when treating individuals with SAPS or other similar conditions.
Reference:
Liaghat, B., Ussing, A., Petersen, B. H., Andersen, H. K., Barfod, K. W., Jensen, M. B., Hoegh, M., Tarp, S., Juul-Kristensen, B., & Brorson, S. (2021). Supervised training compared with no training or self-training in patients with Subacromial Pain Syndrome: A systematic review and meta-analysis. Archives of Physical Medicine and Rehabilitation, 102(12). https://doi.org/10.1016/j.apmr.2021.03.027
by ptfadmin | Mar 6, 2024 | Health Tips
Reviewed by: Zachary Stango, SPT; Bridget Collier, PT, DPT
Temporomandibular disorders (TMD) are characterized by dysfunctions within the temporomandibular joint and/or surrounding masticatory musculature and tissue of the head and neck. The incidence of temporomandibular disorders can plague the affected individuals at random, with treatment consisting of analyzing the insidious onset of those aggravating factors. This has led to research suggesting the use of home exercise protocols for mitigation measures of TMD, with evidence also favoring the use of manual therapy as an effective treatment strategy. The randomized controlled trial conducted by Tuncer et al. (2013) aimed to analyze the effects of manual therapy, along with a home exercise program, for the treatment of temporomandibular related pain and mouth opening dysfunction.
The inclusion criteria for this study consisted of individuals diagnosed with myogenous TMD or anterior disc displacement with reduction, which is characterized by tenderness to palpation of the temporalis and masseter, and painful clicking or crepitus upon opening and closing of the mouth, respectively. Individuals who did not meet those TMD diagnoses were still included if their TMJ pain was occurring for at least 3 months. A total of 40 participants completed this trial, of which were randomly assigned to a group solely completing a home exercise program, or a group completing a home exercise program with an additional manual therapy component. The home exercise program provided to both groups consisted of a multitude of educational components on ergonomics, pain, breathing, posture, and repetitive mandibular exercises focusing on opening and closing of the mouth, as well as medial and lateral gliding of the jaw. The manual therapy group completed the same home exercise program, with the addition of manual-based interventions focused on soft tissue mobilization of the masticatory muscles, gentle jaw isometrics, TMJ and cervical traction, and stretching of the surrounding musculature. The interventions in each group were assigned three times a week for four weeks, with pain and maximal mouth opening serving as the primary outcomes measured.
Pain was measured using the visual analogue scale and analyzed with the participant at rest (defined as pain during the mandible’s resting position), and with stress (defined as pain when chewing gum for one minute, designed to mimic daily chewing habits). Maximal mouth opening was measured in millimeters by asking the participants to open their mouths as wide as possible in a pain-free range. All parameters significantly decreased within each group, but the reductions in visual analogue pain scores and improvements in mouth opening were significantly higher within the group completing both a home exercise program and manual therapy. On average, the group undergoing the manual therapy and home exercises had point reductions of 22.5 for visual analogue scores at rest and 55.5 for visual analogue scores with stress, compared to a 13.0 and 23.0 point reduction, respectively, for the group completing only home exercises. Smaller, but significant, numeric differences were observed in the millimeters of maximal mouth opening, as the manual therapy group displayed an average of a 5.8mm improvement compared to 2.4mm improvement with the home exercise group.
Clinical Bottom Line:
The results of this study serve as evidence that treatment interventions for TMD should consist of a manual therapy component in conjunction with home exercise protocols in reducing pain and restoring mandibular kinematics. These interventions suggest the clinical benefit of skilled therapy services when compared to a biomedical alternative or self-management model, as large variations in the etiology of temporomandibular pain and dysfunction can be assessed and addressed by trained physical therapists.
References:
Tuncer AB, Ergun N, Tuncer AH, Karahan S. Effectiveness of manual therapy and home physical therapy in patients with temporomandibular disorders: A randomized controlled trial. J Bodyw Mov Ther. 2013;17(3):302-308. doi:10.1016/j.jbmt.2012.10.006
by ptfadmin | Feb 29, 2024 | Health Tips
The Effect of Combined Kinematic Chain Exercise on Physical Function, Balance Ability, and Gait in Patients with Total Knee Arthroplasty: A Single-Blind Randomized Controlled Trial Reviewed by: Zachary Stango, SPT; Bridget Collier, PT, DPT
Reviewed by: Zachary Stango, SPT; Bridget Collier, PT, DPT
Protocols regarding the rehab process for total knee arthroplasties (TKA) are consistently analyzed as the growing number of these surgical procedures is expected to increase with the rising population of older adults. Open chain movements, characterized by distal on proximal motion (aka, exercises in which the body part farthest from your body, usually your hand or foot, is moving and not fixed: seated leg extension machine, for example), are often utilized post-operatively to improve strength and ROM of the surrounding musculature without overloading the affected joint. Closed chain exercises, characterized by proximal on distal motion (aka, exercises in which the body part farthest from your body, usually your hand or foot, is fixed and not moving: squats, for example) can be introduced post-operatively to improve weight-bearing and proprioceptive abilities of the affected joint. The randomized controlled trial conducted by An et al. (2023) aimed to analyze the effects of incorporating combined (closed and open) kinematic chain exercises on improving physical function, balance, and gait in the early phases of rehab for individuals undergoing a total knee arthroplasty.
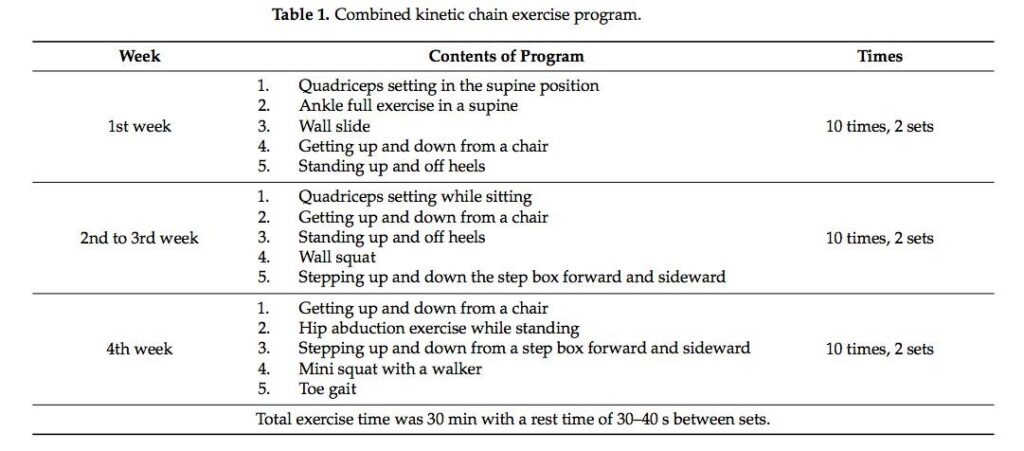
The inclusion criteria for this study consisted of patients aged 65 years or older who underwent a cemented TKA due to osteoarthritic changes. 40 women were randomly assigned to complete a specific kinematic intervention consisting of open or combined chain exercises for 30 minutes five times a week. The interventions were initiated the 3rd day following the surgery and lasted for 4 weeks. The individuals in the combined exercise group completed interventions targeting the hip, knee, and ankle in open and closed chain positions, while the individuals in the open exercise group solely completed the interventions without a load bearing component on the affected knee. Table 1 displays the interventions designed for the group undergoing the combined circuit of open and closed exercises.
A multitude of scales were employed to assess the metrics of this trial. To analyze the effect of the exercise programs on physical function, the trial utilized the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), the Knee Outcome Survey-Activities of Daily Living (KOS-ADL), and range of motion measurements. To analyze balance and gait, the trial used the Zebris PDM platform which is composed of force plates that measured the amount of postural sway of the participants, as well as gait parameters like velocity, cadence, step length, and stride length. The Timed Up and Go (TUG) was also used as a tool to encompass all of the outcomes analyzed: mobility, balance, and gait. In all of the examined outcomes, the combined kinematic chain exercise group produced significant improvements compared to that of the open chain kinematic group.
Clinical Bottom Line:
The results of this trial serve as evidence suggesting the inclusion of closed kinematic chain exercises in conjunction with open kinematic chain exercises, when tolerable, as a vital part of the early phases of the rehabilitation process for patients who have undergone a TKA. The additional weight-bearing component that closed chain exercises provide can be pivotal post-operatively in training the affected joint’s sensory input and surrounding musculature, aiding in the stability of the knee. These improvements are valuable for discussions regarding the patients return to their prior level of function, as the enhancements shown in the results of this trial can be used to ultimately aspire for a reduction in falls and kinesiophobia of patients undergoing this transformative surgery.
References:
An J, Son YW, Lee BH. Effect of Combined Kinematic Chain Exercise on Physical Function, Balance Ability, and Gait in Patients with Total Knee Arthroplasty: A Single-Blind Randomized Controlled Trial. Int J Environ Res Public Health. 2023;20(4):3524. Published 2023 Feb 16. doi:10.3390/ijerph20043524