Effectiveness and cost-effectiveness of individualized progressive walking and education to prevent low back pain recurrence
Reviewed by: John Baur, PT, DPT, OCS, FAAOMPT
Takeaways
- The walking plus education program reduced activity-limiting low back pain recurrence by 28% relative to no treatment.
- Median time to activity-limiting recurrence increased from 112 days in the control group to 208 days in the intervention group.
- Care-seeking recurrence was reduced more strongly than any recurrence, supporting a practical self-management benefit.
- The program had a 94% probability of being cost-effective at a willingness-to-pay threshold of AU$28,000 per QALY.
- Lower extremity adverse events were more common with the intervention, so progression should be individualized and monitored.
Visual Summary of Key Findings
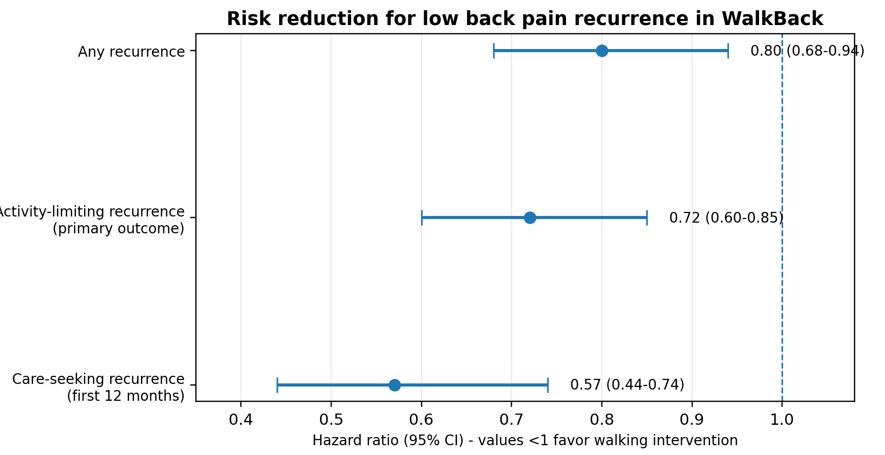
Figure 1. Hazard ratios for the three recurrence outcomes. Values below 1.0 favor the walking and education intervention.
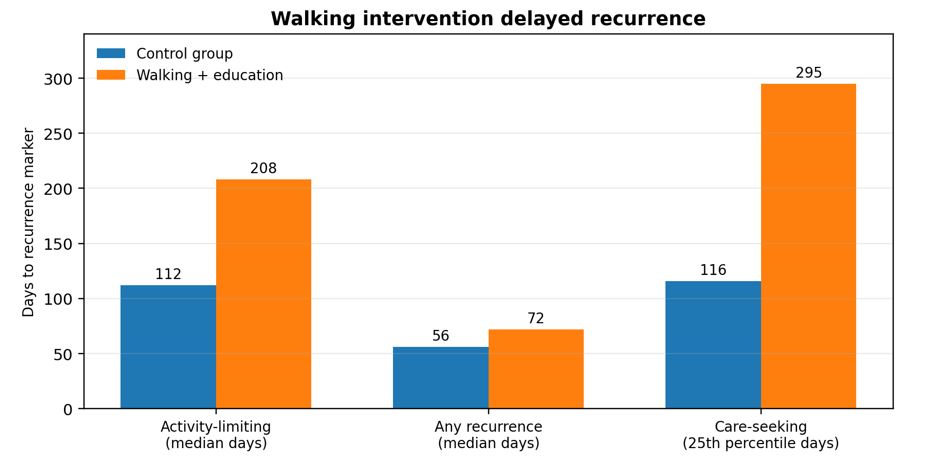
Figure 2. Time-to-recurrence markers reported in the WalkBack trial. Care-seeking recurrence used the 25th percentile because fewer than 50% of intervention participants experienced that event.
Pocovi and colleagues report the WalkBack trial, a pragmatic, two-arm randomized controlled trial designed to test whether a simple, scalable walking and education program could prevent recurrence of non-specific low back pain after recovery. The study addresses an important clinical gap: low back pain is common, recurrent, and costly, yet many prevention programs that combine exercise and education require supervised classes, equipment, or ongoing clinician contact. Walking is inexpensive, familiar, and broadly accessible, but before this trial its effectiveness for preventing low back pain recurrence had not been established in a randomized trial.1
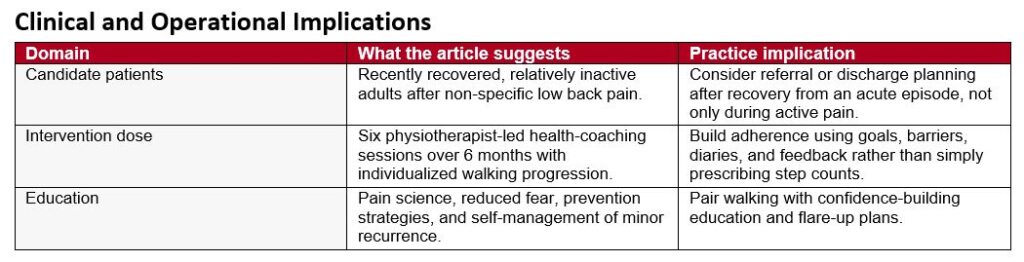
The investigators recruited adults across Australia who had recovered from a recent episode of non-specific low back pain lasting at least 24 hours, with pain greater than 2 on a 0-to-10 scale and at least some interference with day-to-day activities. Recovery was defined as more than 7 consecutive days with pain no greater than 1 out of 10. Key exclusions included comorbidities that prevented walking, current regular walking for exercise, participation in another low back pain prevention program, already meeting moderate or vigorous physical activity guidelines, recent spinal surgery, pregnancy, or inadequate English for study questionnaires. This eligibility approach means the study is most applicable to recently recovered, relatively inactive adults rather than to people with chronic persistent back pain or those already exercising regularly.
A total of 701 participants were randomized: 351 to the intervention and 350 to a no-treatment control group. Participants were predominantly female (81%), and the mean age was 54 years. The intervention consisted of six sessions with a registered physiotherapist over 6 months, with the first five sessions occurring in the first 12 weeks and a booster session at 6 months. The physiotherapist acted as a health coach, helping each participant set a progressive, individualized walking plan. The guiding target was walking 30 minutes per day, 5 days per week by 6 months, but dosing and progression were adapted to baseline activity, age, body mass index, comorbidities, confidence, goals, time constraints, and environmental factors. Participants also received a pedometer and a walking diary for the first 12 weeks.
Education was deliberately paired with the walking prescription. The education component emphasized modern pain science, reduction of fear related to low back pain, practical strategies to reduce recurrence risk, and self-management of minor flare-ups. This pairing is clinically important because recurrent low back pain is not only a mechanical problem; fear, avoidance, low self-efficacy, and uncertainty about safe activity can all influence behavior. The physiotherapists were trained in health coaching, including open-ended questioning, active listening, motivational interviewing, participant-led goal setting, and strategies to promote self-efficacy. Because the trial was disrupted by COVID-19 restrictions, many sessions were delivered by telehealth, which ultimately broadened recruitment across metropolitan, regional, rural, and remote areas.
The primary outcome was time from randomization to the first recurrence of activity-limiting low back pain. Recurrence was measured monthly and defined as a new episode lasting at least 24 hours, with pain intensity greater than 2 out of 10 and at least somewhat interfering with daily activities. Secondary recurrence outcomes were any recurrence and care-seeking recurrence. Additional outcomes included disability, health-related quality of life, physical activity, sedentary behavior, use of co-interventions, adverse events, and cost-effectiveness from a societal perspective. The intention-to-treat analysis and regular monthly follow-up strengthened the time-to-event design and reduced the likelihood of major recall error.
The main clinical result was clear: the walking and education intervention reduced risk of activity-limiting recurrence. The hazard ratio was 0.72 (95% CI, 0.60-0.85; p=0.0002), which corresponds to a 28% relative reduction in recurrence risk. Median time to recurrence was 208 days in the intervention group compared with 112 days in the control group, nearly doubling the time before half of participants experienced an activity-limiting recurrence. The intervention also reduced any recurrence (HR, 0.80; 95% CI, 0.68-0.94; p=0.0066) and care-seeking recurrence during the first 12 months (HR, 0.57; 95% CI, 0.44-0.74; p<0.0001). For care-seeking recurrence, the 25th percentile time to recurrence was 295 days in the intervention group compared with 116 days in the control group, suggesting a particularly meaningful reduction in episodes that drove health care use.
Secondary outcomes supported the primary findings. Back pain-related disability, measured with the Roland-Morris Disability Questionnaire, favored the intervention at every measured time point through 12 months. Differences were modest but consistent, with a 12-month between-group mean difference of -1.28 points. At 3 months, accelerometer data showed that the intervention group took 611 more steps per day, 616 more brisk steps per day, and accumulated 6.4 more minutes per day of moderate-to-vigorous physical activity. Self-reported walking was also higher at 3 months by about 51 minutes per week, although this difference was no longer present at 12 months. That attenuation may reflect increased walking in the control group, reduced ongoing clinician support after the early intervention period, discontinuation of walking diaries, the impact of lower extremity symptoms, or broader pandemic-related changes in walking behavior.
The economic evaluation is one of the article’s most practice-relevant contributions. The intervention cost AU$414 per participant to deliver. From the societal perspective, mean cost per participant was higher in the intervention group than control group, but the intervention generated more quality-adjusted life-years and fewer activity-limiting recurrences. The incremental cost-effectiveness ratio was AU$7802 per QALY gained, and the authors reported a 94% probability of cost-effectiveness at a willingness-to-pay threshold of AU$28,000 per QALY. The cost per participant prevented from having an activity-limiting recurrence was AU$1120. These findings suggest that the intervention is not merely clinically effective but potentially attractive for health systems seeking low-cost prevention strategies.
Safety findings were generally reassuring but require clinical attention. The proportion of participants with at least one adverse event was similar across groups (52% in the intervention group and 54% in the control group), and serious adverse events were also similar (11% vs 10%). However, lower extremity-related adverse events occurred more often in the intervention group, with 100 events reported among 72 participants compared with 54 events among 41 participants in the control group. This pattern is plausible for a walking intervention and reinforces the need for individualized progression, attention to footwear and terrain, monitoring for early lower limb symptoms, and modification rather than rigid adherence when irritability develops.
Several limitations temper interpretation. Participants and treating physiotherapists could not be masked, and several outcomes were self-reported, which may introduce expectation or reporting bias. Generalizability is limited because most participants were women, most were middle-aged or older, ethnicity was not collected, questionnaires required English, and people who were already physically active were excluded. The control group received no structured intervention, so the trial estimates effectiveness against usual nonintervention rather than against an attention-matched education or exercise comparator. Finally, because walking and education were delivered together, the study cannot determine whether the walking prescription, pain education, health coaching, or their combination was the active driver of benefit.
Overall, the WalkBack trial provides strong evidence that a modest number of health-coaching sessions supporting individualized progressive walking, combined with education, can delay recurrence of low back pain and reduce care-seeking episodes in recently recovered, inactive adults. The intervention aligns well with modern guideline principles that emphasize active self-management, reassurance, graded activity, and avoidance of unnecessary medicalization. Its accessibility, compatibility with telehealth, low delivery cost, and favorable cost-effectiveness profile make it a practical candidate for implementation after recovery from an acute low back pain episode. Clinicians should frame walking as a progressive, individualized prevention strategy rather than a generic instruction to walk more, and should pair it with education that builds confidence, reduces fear, and equips patients to manage minor recurrences without overreacting or withdrawing from activity.

Figure 3. Practical implementation model for the WalkBack intervention based on the article description.
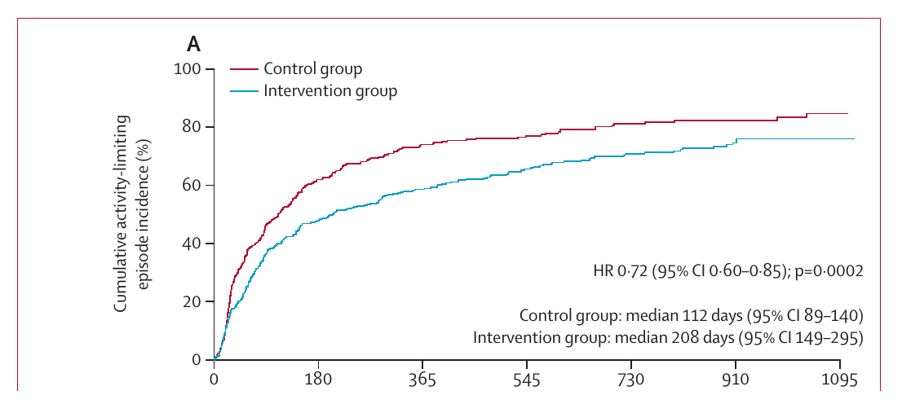
Figure 4. Article Figure 2A excerpt showing cumulative incidence of the primary activity-limiting recurrence outcome. Reproduced from Pocovi et al. under CC BY 4.0.

Reference
- Pocovi NC, Lin C-WC, French SD, et al. Effectiveness and cost-effectiveness of an individualised, progressive walking and education intervention for the prevention of low back pain recurrence in Australia (WalkBack): a randomised controlled trial. Lancet. 2024;404:134-144. doi:10.1016/S0140-6736(24)00755-4