by ptfadmin | Mar 6, 2024 | Health Tips
Reviewed by: Zachary Stango, SPT; Bridget Collier, PT, DPT
Temporomandibular disorders (TMD) are characterized by dysfunctions within the temporomandibular joint and/or surrounding masticatory musculature and tissue of the head and neck. The incidence of temporomandibular disorders can plague the affected individuals at random, with treatment consisting of analyzing the insidious onset of those aggravating factors. This has led to research suggesting the use of home exercise protocols for mitigation measures of TMD, with evidence also favoring the use of manual therapy as an effective treatment strategy. The randomized controlled trial conducted by Tuncer et al. (2013) aimed to analyze the effects of manual therapy, along with a home exercise program, for the treatment of temporomandibular related pain and mouth opening dysfunction.
The inclusion criteria for this study consisted of individuals diagnosed with myogenous TMD or anterior disc displacement with reduction, which is characterized by tenderness to palpation of the temporalis and masseter, and painful clicking or crepitus upon opening and closing of the mouth, respectively. Individuals who did not meet those TMD diagnoses were still included if their TMJ pain was occurring for at least 3 months. A total of 40 participants completed this trial, of which were randomly assigned to a group solely completing a home exercise program, or a group completing a home exercise program with an additional manual therapy component. The home exercise program provided to both groups consisted of a multitude of educational components on ergonomics, pain, breathing, posture, and repetitive mandibular exercises focusing on opening and closing of the mouth, as well as medial and lateral gliding of the jaw. The manual therapy group completed the same home exercise program, with the addition of manual-based interventions focused on soft tissue mobilization of the masticatory muscles, gentle jaw isometrics, TMJ and cervical traction, and stretching of the surrounding musculature. The interventions in each group were assigned three times a week for four weeks, with pain and maximal mouth opening serving as the primary outcomes measured.
Pain was measured using the visual analogue scale and analyzed with the participant at rest (defined as pain during the mandible’s resting position), and with stress (defined as pain when chewing gum for one minute, designed to mimic daily chewing habits). Maximal mouth opening was measured in millimeters by asking the participants to open their mouths as wide as possible in a pain-free range. All parameters significantly decreased within each group, but the reductions in visual analogue pain scores and improvements in mouth opening were significantly higher within the group completing both a home exercise program and manual therapy. On average, the group undergoing the manual therapy and home exercises had point reductions of 22.5 for visual analogue scores at rest and 55.5 for visual analogue scores with stress, compared to a 13.0 and 23.0 point reduction, respectively, for the group completing only home exercises. Smaller, but significant, numeric differences were observed in the millimeters of maximal mouth opening, as the manual therapy group displayed an average of a 5.8mm improvement compared to 2.4mm improvement with the home exercise group.
Clinical Bottom Line:
The results of this study serve as evidence that treatment interventions for TMD should consist of a manual therapy component in conjunction with home exercise protocols in reducing pain and restoring mandibular kinematics. These interventions suggest the clinical benefit of skilled therapy services when compared to a biomedical alternative or self-management model, as large variations in the etiology of temporomandibular pain and dysfunction can be assessed and addressed by trained physical therapists.
References:
Tuncer AB, Ergun N, Tuncer AH, Karahan S. Effectiveness of manual therapy and home physical therapy in patients with temporomandibular disorders: A randomized controlled trial. J Bodyw Mov Ther. 2013;17(3):302-308. doi:10.1016/j.jbmt.2012.10.006
by ptfadmin | Feb 29, 2024 | Health Tips
The Effect of Combined Kinematic Chain Exercise on Physical Function, Balance Ability, and Gait in Patients with Total Knee Arthroplasty: A Single-Blind Randomized Controlled Trial Reviewed by: Zachary Stango, SPT; Bridget Collier, PT, DPT
Reviewed by: Zachary Stango, SPT; Bridget Collier, PT, DPT
Protocols regarding the rehab process for total knee arthroplasties (TKA) are consistently analyzed as the growing number of these surgical procedures is expected to increase with the rising population of older adults. Open chain movements, characterized by distal on proximal motion (aka, exercises in which the body part farthest from your body, usually your hand or foot, is moving and not fixed: seated leg extension machine, for example), are often utilized post-operatively to improve strength and ROM of the surrounding musculature without overloading the affected joint. Closed chain exercises, characterized by proximal on distal motion (aka, exercises in which the body part farthest from your body, usually your hand or foot, is fixed and not moving: squats, for example) can be introduced post-operatively to improve weight-bearing and proprioceptive abilities of the affected joint. The randomized controlled trial conducted by An et al. (2023) aimed to analyze the effects of incorporating combined (closed and open) kinematic chain exercises on improving physical function, balance, and gait in the early phases of rehab for individuals undergoing a total knee arthroplasty.
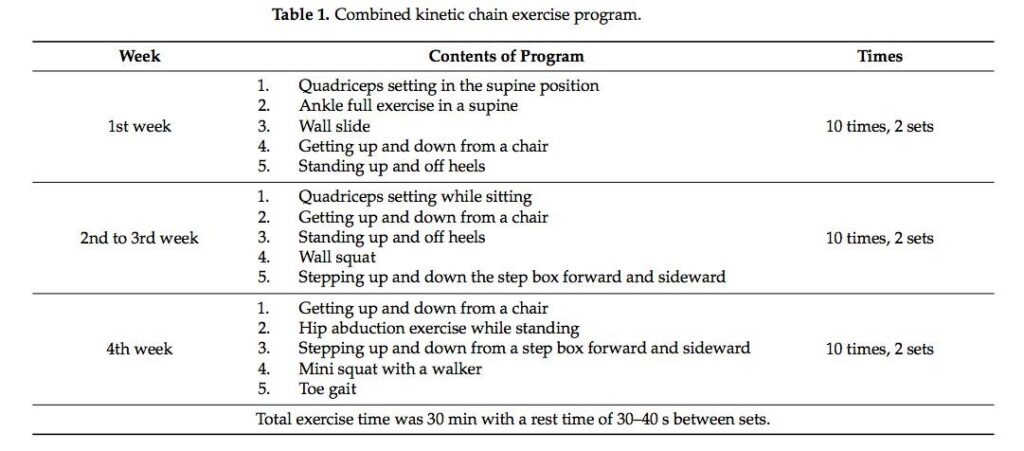
The inclusion criteria for this study consisted of patients aged 65 years or older who underwent a cemented TKA due to osteoarthritic changes. 40 women were randomly assigned to complete a specific kinematic intervention consisting of open or combined chain exercises for 30 minutes five times a week. The interventions were initiated the 3rd day following the surgery and lasted for 4 weeks. The individuals in the combined exercise group completed interventions targeting the hip, knee, and ankle in open and closed chain positions, while the individuals in the open exercise group solely completed the interventions without a load bearing component on the affected knee. Table 1 displays the interventions designed for the group undergoing the combined circuit of open and closed exercises.
A multitude of scales were employed to assess the metrics of this trial. To analyze the effect of the exercise programs on physical function, the trial utilized the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), the Knee Outcome Survey-Activities of Daily Living (KOS-ADL), and range of motion measurements. To analyze balance and gait, the trial used the Zebris PDM platform which is composed of force plates that measured the amount of postural sway of the participants, as well as gait parameters like velocity, cadence, step length, and stride length. The Timed Up and Go (TUG) was also used as a tool to encompass all of the outcomes analyzed: mobility, balance, and gait. In all of the examined outcomes, the combined kinematic chain exercise group produced significant improvements compared to that of the open chain kinematic group.
Clinical Bottom Line:
The results of this trial serve as evidence suggesting the inclusion of closed kinematic chain exercises in conjunction with open kinematic chain exercises, when tolerable, as a vital part of the early phases of the rehabilitation process for patients who have undergone a TKA. The additional weight-bearing component that closed chain exercises provide can be pivotal post-operatively in training the affected joint’s sensory input and surrounding musculature, aiding in the stability of the knee. These improvements are valuable for discussions regarding the patients return to their prior level of function, as the enhancements shown in the results of this trial can be used to ultimately aspire for a reduction in falls and kinesiophobia of patients undergoing this transformative surgery.
References:
An J, Son YW, Lee BH. Effect of Combined Kinematic Chain Exercise on Physical Function, Balance Ability, and Gait in Patients with Total Knee Arthroplasty: A Single-Blind Randomized Controlled Trial. Int J Environ Res Public Health. 2023;20(4):3524. Published 2023 Feb 16. doi:10.3390/ijerph20043524
by ptfadmin | Feb 21, 2024 | Health Tips
Reviewed by Tyler Tice, PT, DPT, OCS, ATC
Introduction:
Arthroscopic partial meniscectomies (APM) are a minimally invasive surgical procedure that is used to reduce or even eliminate the symptoms associated with a meniscus injury. It is common for patients to return to normal recreational activities with very little supervised rehabilitation through physical therapy. However, it is becoming increasingly clear within current evidence that patients who undergo meniscectomy surgeries demonstrate significant quadriceps atrophy, quadriceps inhibition, and strength. Although muscular strength and hypertrophy are common goals of physical therapy after APM, the rate of torque development (RTD) is a metric that is often overlooked in its significance for performing recreational activities and as result many patients maintain a low RTD even 5 weeks post-op. The importance in RTD after APM has not been widely studied and was theorized by the researchers to be heavily linked to patient reported outcomes after surgery because of its role in performance of recreational activity.
Methods:
The study included 20 participants undergoing APM. Participants were excluded from the trial if they had a current or recent other knee ligament injury, recent lower extremity fracture, BMI of 40kg/m2, or inability to perform an MRI. Each participant underwent MRI imaging to determine muscle volume, EMG analysis of quadricep activation, muscle contraction speed testing, knee extension maximal voluntary isometric contraction testing, RTD testing, and voluntary activation completeness.
Conclusions of the Study:
Researchers concluded that there were several factors that contributed to the RTD deficits seen after APM. Maximum strength and the time it takes for the participant to reach maximal strength accounted for roughly 10-15% of the between limb deficits seen in patients after APM. Deficits in neuromuscular control of the quadriceps were a predicted contributor to the slowed RTD seen in APM patients. It was also noted that although a participant may be able to restore quadricep muscle volume and absolute strength after surgery, it does not correlate with a return to previous RTD and deficits in RTD were similar at 2 weeks and 5 weeks post-op to pre-surgical measures. Participants with greater side-to-side differences were associated with worse patient related outcomes, however due to the smaller size of this study and limited scope of time utilized to see patient outcomes these results should be interpreted with caution until a larger study is conducted with the same results.
Clinical Implications:
Quadriceps strength and knee extension range of motion are key aspects of rehab for most post-op knee related patients. However, what is often not considered is the RTD which can be significantly lacking after APM and potentially other arthroscopic surgical interventions. Normal recreational and activities of daily living require a great deal of rapid muscle activation to perform them well. Therefore, it is advised based on the evidence in this study to incorporate rapid knee extension based movement into patient’s rehabilitation program whenever it is appropriate in order to improve RTD. Incorporating knee extension focused power, plyometric, and agility movements, while also promoting quadriceps absolute strength and hypertrophy, could improve patient related outcomes within the first 5 weeks post-op as long as the exercise selection is appropriate for the patient’s goals. However, further investigation is needed in order to determine if there are long term deficits in RTD in APM and other arthroscopic surgical patients that can be addressed by incorporating power, agility, and plyometric training earlier in rehabilitation.
Reference
Cobian, D. G., Koch, C. M., Amendola, A., & Williams, G. N. (2017). Knee extensor rate of torque development before and after arthroscopic partial meniscectomy, with analysis of neuromuscular mechanisms. Journal of Orthopaedic & Sports Physical Therapy, 47(12), 945–956. https://doi.org/10.2519/jospt.2017.7310
by ptfadmin | Feb 15, 2024 | Health Tips
Reviewed by Austin Mowrey PT, DPT
Introduction:
ACL injuries are one of the most common sports-related injuries. After someone suffers an ACL injury they can be classifies as either a coper or non-coper. The term “coper” is utilized to describe someone that can return to prior levels of activity after an ACL rupture without dynamic instability. Previous studies have shown that you are classified as a coper or non-coper based on the Knee Outcome Survey- Activities of Daily Living Scale score ≥80%, global rating scale ≥60%, ≥80% symmetry on the timed hop and ≤ 1 recent episode of giving was during activities of daily living. Non-copers fail to meet one of these criteria. The purpose of this study was to evaluate the consistency of early coper classification before and after 10 sessions of progressive neuromuscular training and strength testing (NMST) in athletes early after acute ACL rupture and to evaluate the association of early coper classification with two-year outcomes.
Methods and Interventions:
This study was the primary analysis of the Delaware-Oslo ACL cohort, a prospective study evaluating athletes after ACL Rupture. 300 subjects participated in the study after the met the following criteria: unilateral ACL rupture confirmed by MRI within seven months of enrollment and regularly participated in level I/II sports prior to injury, had full knee range of motion, minimal effusion, minimal pain, and quadriceps limb symmetry index ≥70% . Participants were excluded if they had a previous injury or surgery on the contralateral knee or significant concomitant injuries. Prior to NMST, participants were identified as copers and non-copers based on the following criteria: Knee Outcome Survey- Activities of Daily Living Scale score ≥80%, global rating scale ≥60%, ≥80% symmetry on the timed hop and ≤ 1 recent episode of giving was during activities of daily living. Non-copers fail to meet one of these criteria. All athletes participated in a 10-session NMST program over approximately 5 weeks, consisting of progressive strengthening, plyometric, and neuromuscular exercises with the goal of restoring muscle strength and neuromuscular control. After the exercise interventions, participants were re-assessed if they classified as copers or non-copers. Success two years after ACLR or non-op rehabilitations was defined as meeting or exceeding sex and age-matched norms on the International Knee Documentation Committee Subjective Knee Form, no ACL graft ruptures and ≤ 1 episode of giving way within the last year.
Results:
Of the 300 athletes who enrolled in the study, 271 completed the post-training data collection. Of the 271 participants that completed the post-training data collection, 219 returned for the two-year follow up. Out of the 219 participants that returned, 93 were ACLR potential copers, 61 were ACLR non-copers, 51 were non-op potential copers and 14 were non-op non-copers.
55% were potential copers at screening and 68% were potential copers at the end of training. 45% of initial potential non-copers become potential copers post-training, while only 13% of initial potential copers become non-copers after training. About 25% of the athletes were non-copers at screening and remained non-copers at the end of training.
At the two year follow-up, 64% of the ACLR group and 74% of the non-op group were successful per the previously described criteria. Using coper classifications at screening, ACLR potential copers had a 2.3 times the odds of success compared to the ACLR non-copers. Non-op potential copers and non-copers did not significantly differ from ACLR non-copers. Using coper classification post-training, ACLR and non-op potential copers had 2.7 and 2.9 times the odds of success compared with ACLR non-copers. The non-op non-copers had 0.51 times the odds of success compared to ACLR non-copers, however it was not statistically significant.
Conclusion:
Nearly 45% of non-copers become potential copers following NMST, while conversion from potential coper to non-coper was 13%. Athletes who were potential copers post-training were more likely to have a successful two-year outcome regardless of operative management compared to the non-copers who received ACLR.
Take Home Message:
- Coper classification can change after NMST.
- Coper classification after a challenge to the neuromuscular system improves insight into two-years outcomes.
- Brief prehabilitation improves long term success.
- Dynamic stability may be more important than mechanical stability for two-year success.
- Alternative strategies are needed for persistent non-copers.
Reference:
Thoma LM, Grindem H, Logerstedt D, et al. Coper Classification Early After Anterior Cruciate Ligament Rupture Changes With Progressive Neuromuscular and Strength Training and Is Associated With 2-Year Success: The Delaware-Oslo ACL Cohort Study. Am J Sports Med. 2019;47(4):807-814. doi:10.1177/0363546519825500
by ptfadmin | Feb 8, 2024 | Health Tips
Reviewed by Mark Boyland PT, DPT, CSCS
Physical Therapists can assist with many patient complaints, and this also includes headaches. This review specifically focused on tension type headaches but there are several headache types. Tension type headaches are classified as headaches which present on both of sides of the head, are non pulsing, mild to moderate intensity, don’t get worse with motion, or may be associated with nausea/vomiting depending on how long you’ve had tension type headaches. Also, those who have tension type headaches may also present with light/noise sensitivity but not both at the same time. Those who have tension type headaches may have at least 10 episodes per year with duration of headaches lasting 30 minutes to 7 days. In short headaches aren’t a pleasant experience especially if they can last upwards of 7 days. Despite our ability to classify headaches we are not exactly sure what causes them which makes treating them a challenge. This review found exactly that, and that while there is no treatment standard in physical therapy for tension type headaches interventions that address the neck, jaw, and thoracic spine are common treatment trends. Not having a standard of treatment provides benefits for our patients as we can customize your treatment plan based on your preferences and dysfunctions as opposed to a cookie cutter model.
This systematic review examined the available trials and found that treatments benefits were divided into short, medium, and long term. While there was no definition provided for short term effects, medium term was defined between 8 weeks and 3 months, and long term was defined as beyond 36 weeks. Treatment interventions included manual therapy including myofascial release of cervical tissues, joint mobilization/manipulation of the cervical and thoracic spine, as well as progressive relaxation of the jaw and cervicothoracic musculature which included patient education as well as other modalities.
With al this said many of the interventions studied had improvements in headache frequency and intensity which is again a good thing for out patients. Unfortunately due to the nature of randomized control trials and systematic reviews the quality of evidence was low for several of the randomized control trials and that no specific recommendations can be made based on their findings. This is the joy of research. However ,with all this said, while many can have tension type headaches, not all symptoms and dysfunctions are the same between all patients and therefore our treatments should be tailored to our patients.
Patient summary: Your therapist will likely address your neck, midback, and jaw during your sessions. You should expect interventions to include manual therapy including soft tissue and joint mobilization will be applied. There’s also going to be some exercises including relaxation, mobilization, and stabilization will be included.
by ptfadmin | Jan 31, 2024 | Health Tips
Reviewed by: Zachary Stango, SPT; Bridget Collier, PT, DPT
The act of raising one’s arm overhead is a simple motion in theory, but biomechanically, it requires a great deal of coordinated motions between a multitude of joints that comprise the shoulder complex. Of the intra-articular motions that occur during arm elevation, upward rotation of the scapula is necessary to allow for full range of motion. Adhesive capsulitis, more commonly known as frozen shoulder, is a common condition that is associated with alterations in the kinematics of the shoulder, contributing to scapular dyskinesis and variations in the amount of upward rotation noted during these motions. Decreased motion of the shoulder is associated with alterations in proprioception of the joint, possibly further contributing to the abnormal rotational movements attributed to this condition. The randomized controlled trial conducted by Mohamed et al. (2020) aimed to analyze the effects of improving awareness of scapular motions on pain, disability, and range of motion in individuals with adhesive capsulitis.
The inclusion criteria for this study consisted of patients with the inability to raise their arm above 100 degrees of scaption, with limitations in both active and passive range of motion interfered by pain. 66 individuals aged 40-60 years old were evenly split into two groups, performing their respective routines for 40 minutes, three times a week for two months while also receiving hot packs and scapular mobilizations. Baseline measurements for shoulder flexion, abduction, external rotation, and scapular upward rotation were noted using an inclinometer. The control group performed active shoulder flexion and abduction exercises, while the experimental group performing dynamic scapular recognition utilized a ViMove motion sensor system, an audible biofeedback device that was placed on the spine of the scapula. The participants performed shoulder abduction, with greater upward rotation of the scapula increasing the sound of the device, providing feedback to the participant that they are performing the desired movement.
Follow up metrics were taken at two weeks, two months, and 6 months following the procedure and the results displayed a significant improvement in upward rotation between the dynamic scapular recognition group compared to the control group at all three timelines. The range of motion values proved to be of similar results, with significant improvements of flexion, abduction, and external rotation of the experimental group noted compared to the control group after 6 months. The Shoulder Pain and Disability Index was the validated measure used to assess pain and disability of the shoulder, with scores exhibiting significant reductions in pain and disability of the experimental group compared to the control group at two weeks and two months. Through the use of the audible biofeedback device, the participants were able to receive active interpretations of their scapular kinematics, perhaps aiding in their joint’s proprioceptive ability to decrease elevation of the scapular prior to the rotational component motions needed to successfully execute full arm elevation.
Clinical Bottom Line:
The results of this trial serve as evidence that biofeedback markers can increase one’s awareness of their compensatory mechanisms and therefore, in this case, can assist in mitigating abnormal kinematics in order to restore proper joint biomechanics. Further research is needed to generalize this theory to other movements that also require a successful synchronicity of the surrounding joints, but this can be trialed as an intervention for those individuals who may respond well to a unique style of cueing.
References:
Mohamed AA, Jan YK, El Sayed WH, Wanis MEA, Yamany AA. Dynamic scapular recognition exercise improves scapular upward rotation and shoulder pain and disability in patients with adhesive capsulitis: a randomized controlled trial [published correction appears in J Man Manip Ther. 2020 Jun 10;:1]. J Man Manip Ther. 2020;28(3):146-158.