Cervicogenic Headaches and Conservative PT
A manual physical therapy approach versus subacromial corticosteroid injection for treatment of shoulder impingement syndrome: a protocol for a randomised clinical trial
Stephanie Racicki, Sarah Gerwin, Stacy DiClaudio, Samuel Reinmann, Megan Donaldson
Introduction:
Headaches are a very common complaint, affecting nearly 47% of the population. Of these headaches, cervicogenic headaches (CGHs) account for ~20% and typically affect women more often than men. This condition can be debilitating and limit your ability to work, sleep, perform household chores, or even ruin the time you want to be relaxing. These types of headaches are very common following a trauma such as whiplash, but just because you may have never been in an auto-accident doesn’t mean you can’t have CGHs. Unfortunately, these can also be caused by the prolonged and poor postures many people assume in their everyday lives.
The International Headache Society (IHS) has classified CGHs as “pain referred from a source in the neck and perceived in one or more regions of the head and/or face”. This means that neck pain usually accompanies the headache, but it is also possible to complain of arm/shoulder pain, dizziness, nausea, lightheadedness, “eye” pain, and visual disturbance.
The next time that you are suffering from a headache, try feeling the back of your neck, specifically right below your skull, to see if there is any muscular tenderness. If so, you may be suffering from a CGH, especially if pressing into these muscles make your headache worse. But the big question is: “What do I do to make my headache go away?”
Review of existing research and literature:
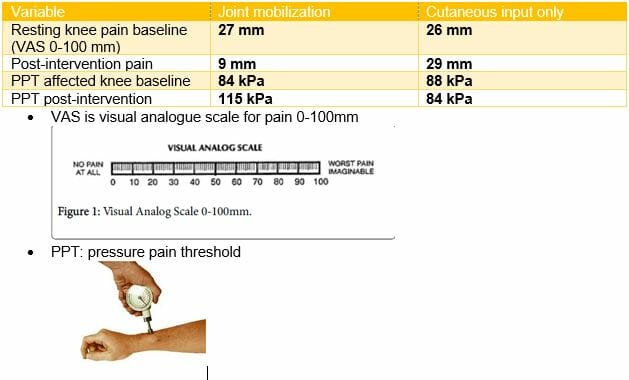
In a systematic review by Racicki et al, researchers attempted to determine the effectiveness of conservative PT approaches to manage patients suffering from cervicogenic headaches. There have been many techniques utilized, including invasive and non-invasive treatments. Invasive approaches can include injections, dry needling, or surgery. Non-invasive treatments can include TENS, massage, mobilization, manipulation, and exercise.
The researchers were able to find a total of 6 articles that fit their criteria which required randomized control trials and an assessment on at least one type of conservative treatment. In these studies, the interventions which were utilized included: cervical manipulation and mobilization, self-mobilization (by the patient), exercise (cerico-scapular strengthening), and thoracic manipulation.
Although the studies reviewed different techniques, many involved similar outcome measures. These included headache frequency, intensity, and duration, as well as disability, neck pain, and amount of analgesic use (pain killers).
Results:
Although the studies assessed different techniques, the overall results demonstrated that the most effective conservative treatments for CGH pain included cervical mobilization and manipulation, as well as exercise to strengthen the cervicoscapular muscles. These were especially helpful in improving headache frequency, intensity, and neck pain.
In addition to the 6 articles that were utilized for this review, the authors reported that some articles that were not included indicated that conservative management could reduce analgesic use as well.
Although this article displayed good success with cervical manipulation and mobilization, the studies included did not report on many of the other conservative treatments that physical therapists offer. These can include deep tissue massage, modalities such as cold packs and TENS, or cervical traction, which could also provide benefits to this patient population.
Conclusion:
Headaches are a common disorder facing many Americans everyday. Conservative physical therapy management, including mobilization, manipulation, and exercise have been shown to have a positive effect on reducing headache intensity, frequency, and neck pain.
If you are suffering from persistent headaches that are affecting your quality of life, physical therapy may be an effective way to reduce your pain and get you back to where you want to be, while teaching self-management techniques to potentially reduce their recurrence.
A manual physical therapy approach versus subacromial corticosteroid injection for treatment of shoulder impingement syndrome: a protocol for a randomised clinical trial
Stephanie Racicki, Sarah Gerwin, Stacy DiClaudio, Samuel Reinmann, Megan Donaldson
Journal of Manual and Manipulative Therapy
2013; Vol. 21 ; No. 2
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3649358/pdf/jmt-21-02-113.pdf