by ptfadmin | Apr 21, 2026 | Health Tips
By Hannah E. Cabre
Reviewed by; John Baur, PT, DPT, OCS, FAAOMPT
Cabre’s narrative review examines how nutrition guidance for strength and conditioning athletes should be adapted for adult, premenopausal cisgender female athletes. The central argument is that sports nutrition practice has advanced faster than the female-specific evidence base. Although women now make up a large share of collegiate sport participation, many calorie, carbohydrate, protein, fat, and supplement recommendations are still extrapolated from studies in men. The review warns that this gap encourages oversimplified advice, including social-media “cycle syncing” claims, and may contribute to inconsistent fueling recommendations that place female athletes at risk for inadequate intake.1
The article first explains that women respond strongly to resistance training. Absolute strength gains are often lower than men’s because of differences in muscle mass and contractile properties, but relative improvements in strength and hypertrophy can be similar, and in some studies greater, in women. Physiologically, women generally have more type I fibers, greater oxidative capacity, better fatigue resistance, and greater reliance on fat oxidation than men, whereas men tend to have greater glycolytic capacity. Estrogen and progesterone fluctuate across the menstrual cycle and can alter substrate use, energy expenditure, recovery, and fluid balance. However, recent evidence suggests that resistance-exercise-stimulated muscle protein synthesis is not meaningfully changed by menstrual cycle phase, so phase-based protein strategies are not supported.
Energy availability is presented as the foundation of health and performance. The review emphasizes Relative Energy Deficiency in Sport (REDs), defined as a mismatch between energy intake and exercise expenditure that can impair metabolism, reproductive function, bone, immune, cardiovascular, and musculoskeletal health. Low energy availability in women is identified as less than 30 kcal per kilogram of fat-free mass per day, while approximately 45 kcal/kg fat-free mass/day is suggested to avoid low energy availability. The author notes that estimating calories for resistance training is difficult because anaerobic work is hard to capture, wearable devices are often inaccurate, and predictive equations should match the athlete’s age, body size, activity level, and life stage. Pregnancy and lactation require special attention because energy and nutrient demands increase, and training may need modification.
For carbohydrates, the review balances performance needs with female-specific metabolism. Carbohydrate remains the primary fuel for high-intensity activity, yet female strength athletes may use less muscle glycogen during resistance exercise than men. Therefore, carbohydrate loading is not automatically necessary. A practical range of 3-7 g/kg/day is recommended depending on training volume, intensity, and daily activity, with 30-60 g/hour during sessions if fatigue limits performance. Carbohydrate supplements can help when food intake is insufficient, but they should not crowd out protein.
Dietary fat is framed as essential for energy density, hormonal function, inflammation control, and recovery. Because women rely more heavily on fat metabolism, adequate fat may be especially important in strength and conditioning contexts. The review recommends at least 15%, and ideally about 20%, of total calories from fat, with approximately 1 g/kg/day during weight maintenance and lower ranges only when supervised fat loss is appropriate. Unsaturated fats and omega-3 intake are emphasized, while trans fats and excessive saturated fats should be limited.
Protein guidance is similar to male athlete recommendations because available evidence suggests comparable protein turnover and muscle protein synthesis responses. Female strength athletes should consume at least 1.5 g/kg/day, within the broader 1.4-2.0 g/kg/day sports nutrition range. The article highlights the value of distributing high-quality protein across the day, targeting essential amino acids and roughly 2.5 g leucine per serving, and consuming 0.32-0.38 g/kg before and after resistance training. A small pre-sleep protein serving may reduce overnight breakdown.
The supplement section focuses on caffeine, creatine monohydrate, and protein powders. Caffeine may support aerobic and anaerobic performance at 3-6 mg/kg about 60 minutes before exercise, although menstrual cycle and contraceptive effects require more study. Creatine is presented as well supported and potentially valuable for women, improving high-intensity power, fatigue measures, cognition, mood, and luteal-phase fluid balance without clear evidence of phase-related weight gain. Protein powders can help meet daily needs when whole foods are limited, especially whey or casein sources rich in leucine.
Overall, the article calls for evidence-based, individualized practice rather than rigid sex stereotypes. Coaches, dietitians, and health practitioners should monitor energy availability, menstrual and pregnancy-related changes, training demands, hunger, fatigue, and recovery. The review’s limitation is the limited female-specific evidence, including small samples, inconsistent menstrual-cycle tracking, and underrepresentation of elite athletes. Its practical contribution is a cautious framework that supports performance while prioritizing long-term health.1
Reference
- Cabre HE. Optimizing performance and health: nutrition considerations for female athletes in strength and conditioning. Strength Cond J. 2025;47(6):619-629.
by ptfadmin | Mar 23, 2026 | Health Tips
Reviewed by Tyler Tice, PT, DPT, OCS, ATC
This scoping review published in Sports Medicine (2024) synthesized literature from 1986–2023, including both published and unpublished studies, to examine the influence of menstrual cycle phases (MCP), menstrual irregularities (MI), and hormonal contraceptive (HC) use on musculoskeletal (MSK) injuries among female athletes aged 13–45 years. The study designs included are as follows: cross-sectional (43), cohort (21), case-control (12), case series (11), case studies (7), and randomized controlled trials (1)
Most studies investigated menstrual irregularities and menstrual cycle phases as injury risk factors. Additionally, most of the research focused on elite or professional-level athletes. Pregnant, perimenopausal, and menopausal women were excluded.
Hormonal Influence on Injury Risk
Injury rates in comparable sports are generally higher among female athletes. Continuous hormonal fluctuations are hypothesized to influence the structure and mechanical properties of muscle, tendon, bone, and ligaments. Both menstrual function and hormonal contraceptive use alter endogenous reproductive hormone levels, potentially affecting injury risk. A typical menstrual cycle includes the follicular phase, ovulation, and the luteal phase respectively. Hormonal fluctuations throughout these phases have been associated with increased risk of both acute and overuse injuries.
In female soccer players, injury incidence appears greatest during the late follicular phase. Increased risk of muscle, tendon, and anterior cruciate ligament (ACL) injuries has also been observed during this phase. Additionally, peak estrogen levels during ovulation are associated with increased ligament laxity, altered strength, and reduced neuromuscular control, which may predispose athletes to injury. However, findings across studies are inconsistent, and a direct causal relationship between menstrual cycle phase and injury has not been definitively established.
Menstrual Irregularities and Injury
Menstrual irregularities are prevalent among female athletes and are associated with elevated injury risk. High school athletes with menstrual dysfunction demonstrate greater time-loss severity compared to athletes with regular menstrual cycles.
The Female Athlete Triad, now referred to as Relative Energy Deficiency in Sport (RED-S), highlights the interrelationship between low energy availability, menstrual dysfunction, and reduced bone mineral density. RED-S also has implications for cardiovascular health, immunity, metabolic rate, and overall menstrual function. Athletes with menstrual irregularities are particularly susceptible to bone stress injuries due to reduced estrogen levels and compromised bone health.
Hormonal Contraceptives and Injury Risk
Approximately half of female athletes use hormonal contraceptives, including: oral contraceptive pills (OCPs), intrauterine devices (IUDs), injections, transdermal patches, implants, and vaginal rings. Hormonal contraceptives suppress endogenous hormone production and eliminate typical cyclical fluctuations. Some literature included in this review suggests that hormonal contraceptives, particularly oral contraceptives, may provide a protective effect against injury. Among female athletes, some studies suggest that oral contraceptive use, with or without neuromuscular training, may improve dynamic knee stability and potentially reduce ACL injury risk. However, evidence from the general population indicates that combined hormonal contraceptives are not protective against MSK injuries.
Overall, evidence remains inconclusive due to methodological variability across studies. Despite inconsistencies in the literature, physical therapists should not dismiss menstrual and hormonal influences, as they may represent an important piece of the multifactorial puzzle in injury risk and rehabilitation for female athletes.
Reference:
MacMillan, C., Olivier, B., Viljoen, C. et al. The Association Between Menstrual Cycle Phase, Menstrual Irregularities, Contraceptive Use and Musculoskeletal Injury Among Female Athletes: A Scoping Review. Sports Med 54, 2515–2530 (2024). https://doi.org/10.1007/s40279-024-02074-5
by ptfadmin | Mar 16, 2026 | Health Tips
Reviewed by Tyler Tice, PT, DPT, OCS, ATC
This double-blind randomized control trial aimed to assess the clinical effects of Kinesiotape (KT) regarding short term use on rotator cuff tendinopathy (RCT). KT is a conservative treatment for rotator cuff pathologies, inspired by traditional Japanese medicine. The tape is made with impermeable and non-degradable in water materials and is without ant added chemicals. KT provides traction to the skin, which may result in reduction of pressure on mechanoreceptors, providing relief to affected muscle and joint systems. Additionally, it is thought that KT improves blood and lymphatic circulation, however the pathophysiological mechanism is not fully understood.
Inclusion criteria for this study were: age between 20 and 60 years, shoulder pain before 150° of active elevation in any plane, pain during resisted external rotation, abduction or empty can test, and positive signs of conflict (Neer’s or Hawkins sign) on clinical examination. Patients were excluded if they had: progressive dermatological pathology, history of surgery, fracture or dislocation of shoulder, local corticosteroid infiltration in the previous 6 months, reproduction of symptoms during the cervical screening examination, cervical radiculopathy, or hyperpilosis that may impede the application of KT. Examination via Ultrasound was conducted to identify potential anatomical lesions (simple tendonitis, bursitis, calcification, or partial tear). Patients that unknowingly had a tear on the affected side were excluded.
Subjects were randomized into two groups. Standardized KT for shoulder pain (n=25) and sham KT application (n=25). Patients were instructed to maintain ADLs, but to avoid adding any new physical activity into their daily routine and to avoid analgesic therapy as much as possible. Both groups received 3 KT applications that were 4 days apart. The subjects were informed that two different techniques were used, but other details were withheld. For the KT group: a “Y”shaped strip was placed at the deltoid, from its insertion to its origin. The first tail of the band was applied to the anterior deltoid, with the patient’s arm in 60–80° horizontal abduction and complete external rotation, while the second tail was applied to the posterior deltoid, with the arm in 20–30° horizontal adduction and complete internal rotation. Additionally, an “I” strip was placed at supraspinatus muscle, applied from its insertion to its origin, with lateral cervical flexion to the opposite side and with the arm held behind the back. See below for the sham application.

The DASH was used to determine outcomes. Repeat-measures ANOVA were used to analyze the data. both groups demonstrated significant DASH score improvements and VAS reports.
Limitations of this study include: shoulder ROM was not assessed, absence of a no-tape control group, various pathologies amongst the sample, and many patients reduced activity levels despite instructions.
As physical therapists, it is important that we do our best to strive for positive patient outcomes while promoting patient independence and ownership of their condition. KT is a potential short term intervention that could be used as an adjunct treatment to facilitate decreased pain levels and in turn, more patient buy-in for physical therapy. However, the main treatment focus should consist of: progressive loading, therapeutic exercise, and patient education to promote long-term independence and functional recovery.
References:
Taik FZ, Karkouri S, Tahiri L, et al. Effects of kinesiotaping on disability and pain in patients with rotator cuff tendinopathy: double-blind randomized clinical trial. BMC Musculoskelet Disord. 2022;23(1):90. Published 2022 Jan 26. doi:10.1186/s12891-022-05046-w
by ptfadmin | Mar 9, 2026 | Health Tips
Reviewed by Tyler Tice, PT, DPT, OCS, ATC
This systematic review evaluated the clinical and preclinical evidence for cannabidiol (CBD), excluding THC, as a treatment for pain. The study followed PRISMA guidelines and searched PubMed and Web of Science using the terms “((cannabidiol) NOT (THC)) NOT (tetrahydrocannabinol)) AND (pain treatment)”. Inclusion criteria consisted of clinical and preclinical trials (in vitro and in vivo) in which CBD was used alone or as the major component of cannabis in any pharmaceutical form and free of THC. A total of 40 studies met inclusion criteria, including 11 human clinical trials, 2 canine clinical trials, and 27 preclinical studies. Exclusion criteria included the presence of THC or other cannabis components, systematic or narrative reviews, meta-analyses, case reports, and articles not published in English or Spanish. Literature screening was conducted independently by two researchers and supervised by a third reviewer
Cannabis (hemp) has been used for thousands of years for textile, medicinal, and culinary purposes. The primary compounds of pharmaceutical interest are cannabinoids, with CBD demonstrating a wide range of pharmacologic effects, including anti-inflammatory, antioxidant, anticonvulsant, and antipsychotic properties, mediated through interactions with multiple endogenous receptors. CBD can be administered orally, topically, intravenously, or intraperitoneally. Oral administration was the most common route in clinical trials, while intraperitoneal administration predominated in preclinical studies. One canine clinical trial reported that oral CBD bioavailability was approximately 19% lower compared to other formulations, highlighting the importance of administration route when determining appropriate dosing. The authors emphasized the need for further studies to establish optimal delivery methods based on specific pain pathologies.
Among the human clinical trials, 7 of 11 studies demonstrated pain-reducing effects of CBD. Conditions showing benefit included osteoarthritis, chronic pain, neuropathic pain, bruxism, arthritis, and atopic dermatitis. Importantly, no clinical or preclinical trials reported significant adverse effects or treatment discontinuation. The review concluded that CBD is a potentially effective and safe treatment for pain, supported by its analgesic and anti-inflammatory properties, though larger, well-designed clinical trials are needed to strengthen the evidence base.
Reference:
Cásedas G, Yarza-Sancho M, López V. Cannabidiol (CBD): A Systematic Review of Clinical and Preclinical Evidence in the Treatment of Pain. Pharmaceuticals (Basel). 2024;17(11):1438. Published 2024 Oct 28. doi:10.3390/ph17111438
by ptfadmin | Mar 2, 2026 | Health Tips
Reviewed by Tyler Tice, PT, DPT, OCS, ATC
Background:
- Unilateral vestibular hypofunction( UVH) : partial or complete loss of function in one of the peripheral vestibular organa, and/or nerves
- Acute UVH: most commonly due to vestibular neuritis, but also may be due to trauma, surgical transection, ototoxic meds, or Meniere’s disease.
- Bilateral vestibular hypofunction (BVH): idiopathic in 20-51% of cases
- Common presentation/symptoms:
- dizziness, imbalance, and/or oscillopsia, gaze and gait instability, and impaired navigation and spatial orientation
- Spatial navigation impairments
- Memory, executive function, attention
- Prevalence increases with age
- Higher fall risk
- Typically, bilateral
Population:
vestibular hypofunction
Strong evidence:
Vestibular PT to mitigate symptoms and improve postural stability, gaze, and function
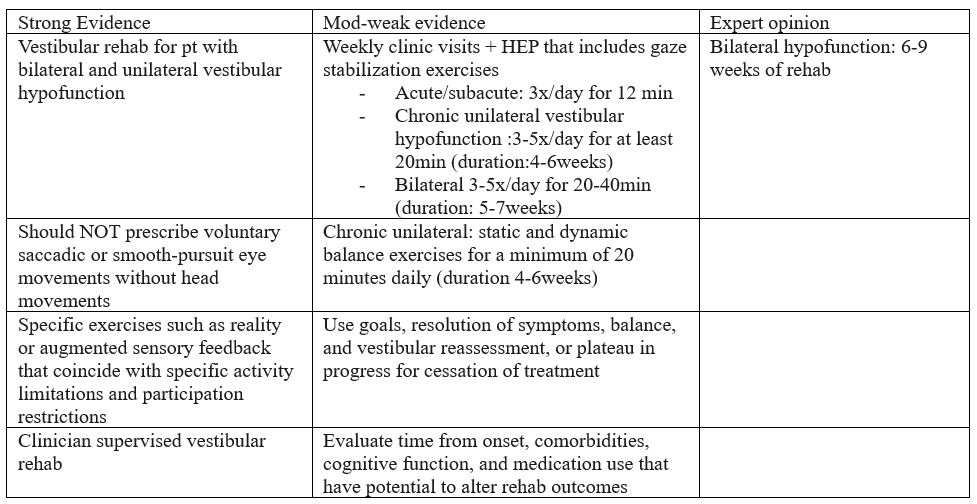
Limitations:
peripheral hypofunction (does not apply to individuals with central disorders)
References:
Hall CD, Herdman SJ, Whitney SL, et al. Vestibular Rehabilitation for Peripheral Vestibular Hypofunction: An Updated Clinical Practice Guideline From the Academy of Neurologic Physical Therapy of the American Physical Therapy Association. J Neurol Phys Ther. 2022;46(2):118-177. doi:10.1097/NPT.0000000000000382