By: Dae Yun Seo, Sung Ryul Lee, Jun-Won Heo, Mi-Hyun No, Byoung Doo Rhee, Kyung Soo Ko, Hyo-Bum Kwak, Jin Han
Reviewed by: John Baur, PT, DPT, OCS, FAAOMPT
Summary
Seo and colleagues review ursolic acid (UA), a naturally occurring pentacyclic triterpenoid found in several fruits, herbs, and plant tissues, including apple peel, rosemary, thyme, lavender, marjoram, organum, flowers, and berries. The article positions UA as a biologically active compound with broad therapeutic potential because it appears to influence inflammation, oxidative stress, apoptosis, metabolism, mitochondrial activity, and muscle protein turnover. The review is organized by organ system and disease category rather than by a single pathway, which is appropriate because UA is presented as a pleiotropic compound whose effects depend heavily on tissue context. At the chemical level, UA is described as 3β-3-hydroxy-urs-12-ene-28-oic acid, with the formula C30H48O3 and molecular mass of 456.71 g/mol. This structural background supports the authors’ broader argument that UA has sufficient molecular complexity to interact with diverse cellular signaling networks.1
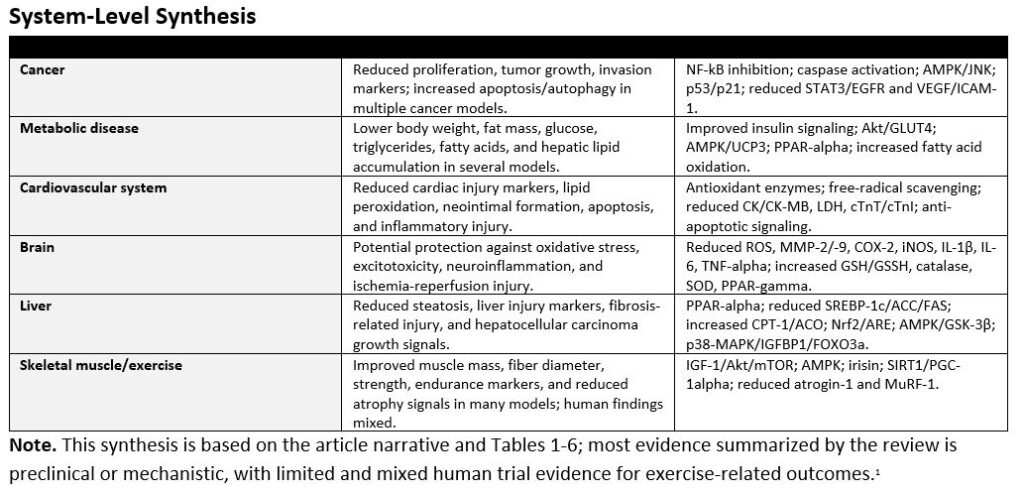
A major theme of the review is UA’s anti-cancer activity. Across skin, colon, breast, bladder, cervical, pancreatic, ovarian, and liver cancer models, the authors summarize evidence that UA can suppress tumor growth, reduce cancer cell proliferation, promote apoptosis, and modulate autophagy. The mechanisms described include inhibition of nuclear factor-kappa B (NF-kB) signaling, reductions in proteins associated with survival and proliferation such as Bcl-2, Bcl-xL, cyclin D1, STAT3, and EGFR, and activation of pro-apoptotic markers such as caspases. UA is also discussed as a regulator of metabolic stress in cancer cells, including AMPK activation and reductions in ATP production, lactate, and glycolytic enzymes. The review’s cancer section is persuasive mechanistically, but it is important to interpret it as mainly preclinical. Much of the cited evidence comes from cell lines and animal models, so the article supports UA as a promising anti-cancer lead compound rather than as an established clinical therapy.1
The article also highlights UA’s potential metabolic benefits in obesity, metabolic syndrome, and diabetes. The authors describe findings in which UA reduced body weight, body mass index, waist circumference, fasting glucose, triglycerides, free fatty acids, fat mass, and hepatic lipid accumulation. Several mechanisms are emphasized: improved insulin signaling, Akt activation, glucose transporter type 4 translocation, AMPK-dependent energy expenditure, increased fatty acid uptake and beta-oxidation, activation of peroxisome proliferator-activated receptor alpha (PPAR-alpha), and modulation of adipocyte transcription factors. One particularly important point is that UA appears to act in multiple metabolically active tissues, including skeletal muscle, adipose tissue, and liver. This makes the compound especially relevant to metabolic syndrome, in which insulin resistance, ectopic fat deposition, inflammation, and altered energy expenditure are interconnected.1
For cardiovascular disease, the review summarizes data suggesting cardioprotective and vasoprotective effects. In animal and cell models, UA was associated with reductions in heart rate, mean arterial pressure, neointimal formation, lipid peroxidation, serum markers of cardiac injury, apoptosis-related cardiac proteins, and inflammatory signaling. The authors emphasize antioxidant defense as a recurring mechanism, including increased activity or availability of superoxide dismutase, catalase, glutathione peroxidase, glutathione reductase, glutathione, and vitamins C and E. These findings suggest UA may protect cardiovascular tissue by reducing oxidative injury and stabilizing enzymes and membranes under ischemic or inflammatory stress. However, as with the cancer literature, the cardiovascular evidence summarized is mainly preclinical. The review therefore provides a mechanistic rationale for future cardiovascular research rather than definitive clinical evidence.1
The brain-focused section presents UA as a neuroprotective compound that may counter oxidative stress, excitotoxicity, neuroinflammation, and apoptosis. The authors discuss models of glioma invasion, D-galactose-induced neurodegenerative changes, subarachnoid hemorrhage, Parkinsonian injury, and cerebral ischemia-reperfusion. Across these models, UA is reported to lower reactive oxygen species, advanced glycation end products, inflammatory mediators, matrix metalloproteinases, and caspase-related apoptotic signaling while increasing antioxidant systems such as glutathione, catalase, and superoxide dismutase. A notable feature of the review is the repeated link between UA and NF-kB-related inflammation, which appears in cancer, brain, and other organ systems. The brain section reinforces the broader concept that UA may protect vulnerable tissues by simultaneously reducing inflammatory signaling and improving antioxidant capacity.1
The liver section is one of the strongest examples of UA’s multi-pathway profile. The authors summarize evidence related to fatty liver disease, hepatic steatosis, liver fibrosis, hepatocellular carcinoma, and liver cancer cell lines. In metabolic liver disease models, UA reduced liver weight, hepatic triglycerides, free fatty acids, liver injury markers such as AST and ALT, and lipogenesis-related factors including SREBP-1c, acetyl-CoA carboxylase, and fatty acid synthase. At the same time, it increased fatty-acid oxidation markers such as carnitine palmitoyltransferase-1 and acyl-CoA oxidase and promoted PPAR-alpha signaling. In fibrosis and cancer models, UA was associated with antioxidant pathways, Nrf2/antioxidant response element activation, apoptosis regulation, AMPK/GSK-3β signaling, p38-MAPK activity, and altered IGFBP1 and FOXO3a expression. These diverse findings support the authors’ conclusion that UA may be relevant to both metabolic and proliferative liver disorders.1
The final major section examines sarcopenia and exercise capacity, where UA is framed as a possible exercise mimetic. The authors describe evidence that UA may increase skeletal muscle mass, muscle fiber diameter, grip strength, exercise time, running distance, swimming duration, mitochondrial biogenesis, and serum or tissue markers related to IGF-1, irisin, Akt/mTOR, AMPK, SIRT1, and PGC-1alpha. UA also appears to reduce muscle atrophy pathways such as atrogin-1 and MuRF-1. This section is clinically appealing because sarcopenia and declining exercise capacity are common problems in aging and chronic disease. However, the review appropriately acknowledges that human data are mixed. Some studies reported improved muscle strength or lower markers of exercise-induced muscle damage, whereas others did not show meaningful changes in muscle mass, function, IGF-1, or Akt/mTOR signaling. This inconsistency makes the exercise-mimetic claim promising but not settled.1
Overall, the article presents UA as a compound with broad potential across cancer, metabolic disease, cardiovascular disease, brain injury, liver disease, sarcopenia, and exercise performance. Its unifying mechanisms include suppression of inflammation, reduction of oxidative stress, regulation of apoptosis and autophagy, improvement of insulin and lipid metabolism, support of mitochondrial function, and modulation of muscle protein turnover. The review’s greatest value is that it integrates findings across organ systems and identifies recurring pathways that may explain UA’s wide range of reported effects. Its major limitation is that many conclusions rely on cell culture or animal studies, with fewer rigorous human trials. Dose, formulation, bioavailability, safety, patient selection, and long-term outcomes remain insufficiently defined. Therefore, UA should be viewed as a promising natural compound for further translational research, not as a proven replacement for established therapies. The most useful next step would be well-designed clinical trials that test standardized UA preparations, clinically meaningful endpoints, and mechanistic biomarkers in specific patient populations.1
Visual Summary
The following visuals highlight how broadly the article organizes the reported effects of ursolic acid (UA). The chart below is a descriptive count of entries in the review tables, not a ranking of evidence quality or clinical certainty.1
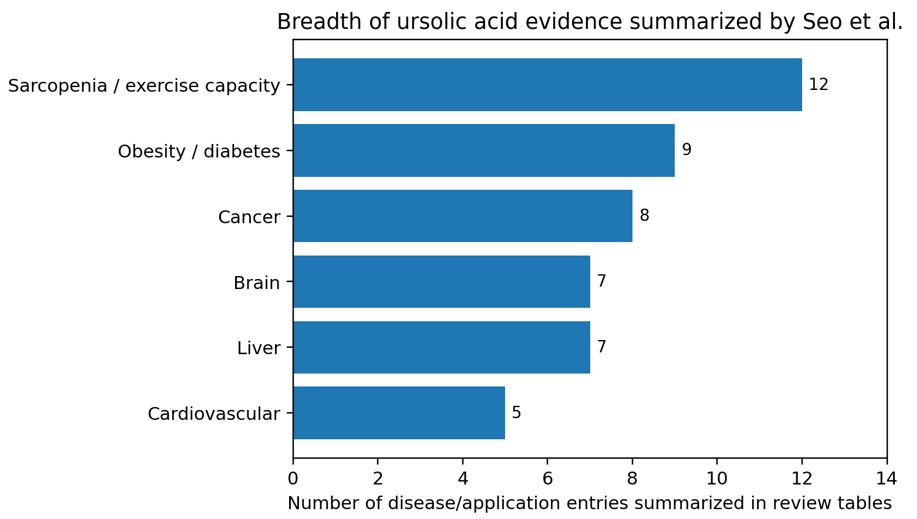
Figure 1. Breadth of disease/application areas represented in the review tables. Counts reflect table entries synthesized by the article and should not be interpreted as clinical strength of evidence.1
Article Figure
The article’s organ-system graphic provides a useful visual summary of UA’s proposed tissue-specific effects and mechanisms.1
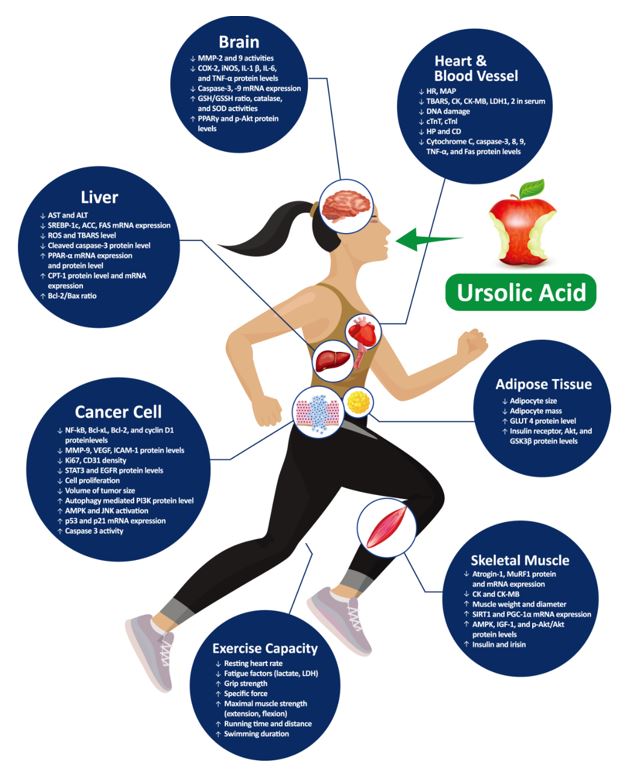
Figure 2. Role of UA in various organs, reproduced from Seo et al. under the article’s open-access license.1
Reference
- Seo DY, Lee SR, Heo JW, et al. Ursolic acid in health and disease. Korean J Physiol Pharmacol. 2018;22(3):235-248. doi:10.4196/kjpp.2018.22.3.235