2024 Clnical Practice Guideline for Midportion Achilles Tendinopathy
Reviewed by: John Baur, PT, DPT, OCS, FAAOMPT
Chimenti and colleagues present the 2024 revision of the Academy of Orthopaedic Physical Therapy clinical practice guideline for Achilles pain, stiffness, and muscle power deficits related specifically to midportion Achilles tendinopathy. The guideline is intended for physical therapists and other clinicians who manage posterior ankle pain and tendon-related functional limitations.1 It updates prior 2010 and 2018 guidance by incorporating literature published through March 7, 2024, with particular emphasis on physical therapy interventions. The authors define tendinopathy as local tendon pain associated with tendon-loading activities, which is important because the term avoids assuming that inflammation or degeneration is the sole cause. The scope is deliberately narrow: it addresses midportion Achilles tendinopathy, typically pain located more than 2 cm proximal to the calcaneal insertion, and does not directly generalize to insertional Achilles tendinopathy.
The guideline frames midportion Achilles tendinopathy as a common, functionally limiting overuse condition affecting athletic and nonathletic populations. The article notes a reported prevalence of approximately 4% to 7%, with higher prevalence associated with increasing age and greater athletic involvement. Runners are highlighted as a particularly relevant population, with prior data suggesting a substantial lifetime chance of Achilles tendon injury. The clinical course is variable. Most individuals improve, but recovery may take months and depends on a combination of biological, functional, psychosocial, and disability-related factors. The authors emphasize that symptom duration alone may not be a strong predictor of response; acute and chronic presentations can both improve with appropriate tendon-loading rehabilitation. Symptom irritability, load tolerance, lower extremity strength and endurance, body mass index, tendon morphology, fear of movement, pain beliefs, and self-efficacy may all influence progress.
Diagnosis remains primarily clinical. The 2024 summary recommends identifying symptoms localized to the Achilles tendon midportion, pain provoked by tendon-loading activities, pain with palpation of the tendon midportion, and tendon thickening when present. The Royal London Hospital test and painful arc sign remain useful examination findings, although localized thickening can be absent in some patients. The guideline also highlights differential diagnosis. Clinicians should reconsider the diagnosis when symptoms do not fit the expected pattern or do not improve with appropriate rehabilitation. Important alternatives include partial Achilles tendon tear, retrocalcaneal or subcutaneous bursitis, posterior ankle impingement, sural nerve irritation, tibial or calcaneal stress fracture, os trigonum syndrome, accessory soleus muscle, Achilles tendon ossification, systemic inflammatory disease, plantaris involvement, paratenonitis, fascial tears, and insertional Achilles tendinopathy.
The article takes a selective approach to imaging. Ultrasound, radiographs, and magnetic resonance imaging can support clinical reasoning when the diagnosis is uncertain, recovery is delayed, symptoms worsen during care, or an invasive procedure is being considered. Imaging is not required for routine diagnosis, and the authors caution that structural findings must be interpreted in context. Increased tendon thickness, for example, is common in symptomatic tendinopathy but can also appear in asymptomatic adults. Ultrasound is presented as accessible, low cost, and useful for visualizing soft tissue, while radiographs help assess bony contributors and MRI is generally reserved for specific diagnostic or procedural planning needs.
The strongest recommendation is for tendon-loading exercise as first-line care. Clinicians should use loading exercises, at the highest load tolerated, to decrease pain and improve function in individuals without presumed tendon-structure frailty. This recommendation is not limited to eccentric training. The CPG uses the broader term tendon loading to include eccentric, concentric, isometric, isotonic, heavy slow resistance, and plyometric loading of the plantar flexors. Evidence summarized in the article indicates that exercise improves pain and function compared with wait-and-see or passive approaches, with clinically meaningful improvements appearing as early as two weeks and commonly reaching approximately 18 to 21 points on the Victorian Institute of Sports Assessment-Achilles scale by 12 weeks. The guideline advises exercise at least three times weekly at an intensity as high as tolerated, while recognizing that clinicians must adjust volume and intensity based on irritability, functional capacity, and total daily tendon load.
Education and counseling are the second core intervention. The authors recommend combining tendon loading with either pain science education or pathoanatomic education. Both approaches can be effective, and delivery may occur in person, by telehealth, or through a hybrid model depending on the patient’s preference. A key message is that complete rest is not indicated. Patients should continue activity within pain tolerance, using symptoms to guide progression rather than avoiding tendon loading entirely. This point is central to the clinical logic of the guideline: recovery is built around graded exposure, confidence, and restoration of load capacity rather than passive protection alone.
Several adjunct interventions may be used selectively, but none replace exercise and education. Stretching may be used when ankle dorsiflexion restriction is present. Neuromuscular re-education may target lower extremity movement impairments that contribute to abnormal Achilles loading. Manual therapy may be applied to muscles, joints, or connective tissues when mobility deficits are present, although the recommendation is based on expert opinion rather than strong clinical trial evidence. Intramuscular dry needling may be considered for calf-related pain and stiffness, especially in more acute cases or when patients cannot yet tolerate progressive loading. Heel lifts may temporarily reduce dorsiflexion demands during activity. Taping may be used to reduce pain, alter foot posture, or reduce tendon strain, but supporting evidence is largely theoretical or indirect. Orthoses remain an area of uncertainty because evidence is contradictory.
The guideline is also explicit about interventions that should not be emphasized. Low-level laser therapy should not be used for midportion Achilles tendinopathy, and therapeutic ultrasound should not be used as a stand-alone treatment. Night splints remain unsupported for improving symptoms. Multimodal treatment may be used to enhance exercise effects, but the article stresses that the best combination of adjuncts is unclear, and many network meta-analysis rankings are limited by small samples, heterogeneity, and risk of bias. Overall, the CPG discourages passive modality-driven care and encourages impairment-based, active rehabilitation.
Outcome measurement is another strength of the article. Clinicians are advised to track patient-reported symptom severity and activity limitations using tools such as the VISA-A, Foot and Ankle Ability Measure, or Lower Extremity Functional Scale. The CPG also points to newer Achilles-specific measures, including the TENDINopathy Severity assessment-Achilles and VISA-A sedentary, which may be useful in nonathletic populations. Physical performance measures such as heel-rise endurance, hop testing, movement-evoked pain during loading, ankle range of motion, plantar flexor strength and endurance, gait, and palpation findings help clinicians document baseline impairment and response to treatment.
The decision tree on pages 18 and 19 translates these recommendations into a practical workflow. It begins with medical screening, proceeds through diagnosis and differential evaluation, then classifies patients by symptom irritability and load tolerance. Patients with low load tolerance may require lower-load tendon exercise, temporary unloading strategies, mobility interventions, and careful symptom monitoring before progressing. Patients with higher load tolerance can generally begin higher-intensity mechanical loading sooner. The guideline’s definition of successful recovery at 6 to 12 months includes a VISA-A score greater than 80, tolerable intermittent pain, resumed primary activities, and achievement of patient goals. If progress is poor, the pathway recommends re-evaluation and referral when needed.
Overall, this 2024 CPG supports a patient-centered, active, and load-progressive approach to midportion Achilles tendinopathy. Its most actionable message is that tendon-loading exercise and education form the foundation of care, while adjuncts should be selected only when they address a specific impairment, symptom barrier, or activity need. The article is methodologically transparent, uses formal evidence grading, and clearly separates strong recommendations from weak, conflicting, theoretical, or expert-opinion guidance. Its main limitations are the incomplete evidence base for acute presentations, sedentary patients, psychosocial subgroups, exercise dose selection, and many adjunct interventions. Nevertheless, the guideline gives clinicians a clear framework: diagnose clinically, avoid unnecessary imaging, keep patients active within tolerance, progressively rebuild tendon capacity, monitor meaningful outcomes, and reserve passive or invasive pathways for situations in which active rehabilitation does not produce adequate improvement.
Visual Synthesis
Figure 1. Distribution of recommendation strength across the article’s 2024 intervention recommendations.
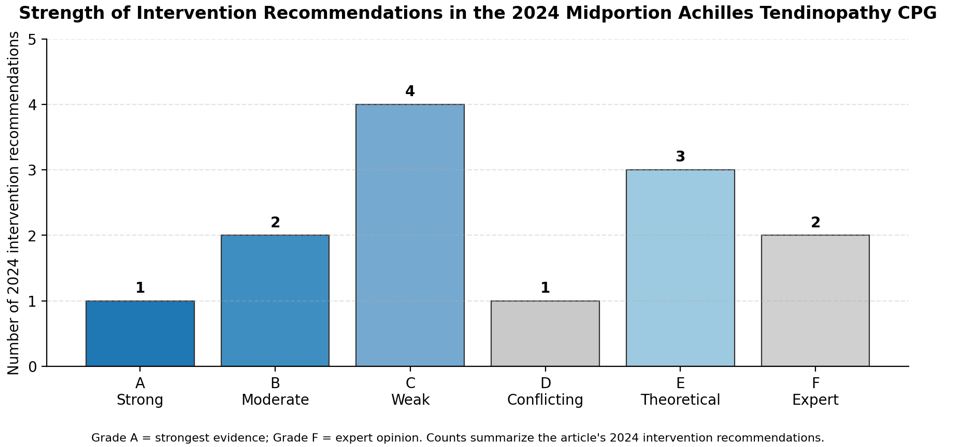
The chart shows that only tendon-loading exercise receives a Grade A recommendation, while several adjunctive strategies remain weak, theoretical, conflicting, or expert-opinion based.
Figure 2. Simplified management pathway based on the guideline decision tree and intervention recommendations.
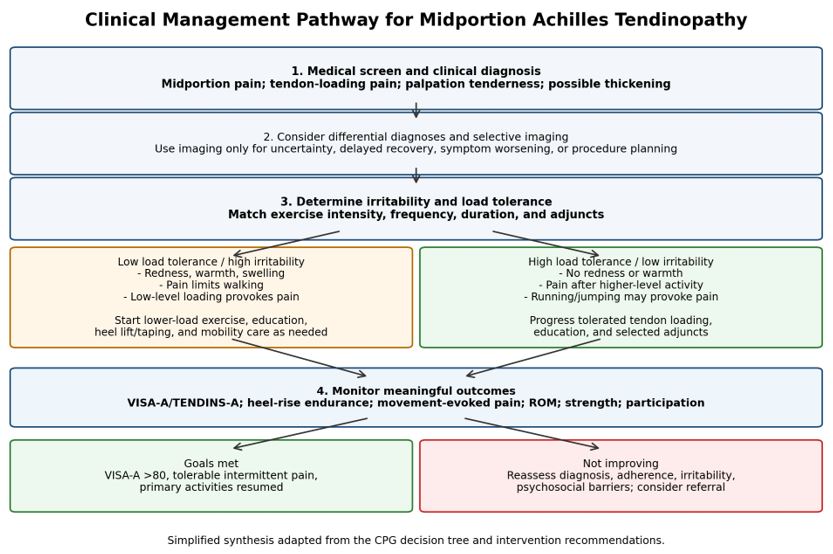
This pathway summarizes the article’s sequence of screening, clinical diagnosis, differential diagnosis, irritability staging, intervention matching, outcome monitoring, and referral or discharge decision-making.
Practical Clinical Takeaways
|
Care Element |
Guideline Direction |
Clinical Implication |
|
Tendon-loading exercise |
Grade A first-line treatment; exercise at least 3 times weekly at high tolerated intensity. |
Build load capacity using eccentric, concentric, isometric, isotonic, heavy slow resistance, and/or plyometric progressions. |
|
Education and activity |
Grade B recommendation to combine education with exercise and avoid complete rest. |
Use pain monitoring, graded exposure, reassurance, and shared decision-making to keep patients active within tolerance. |
|
Adjunctive mobility or symptom tools |
Manual therapy and dry needling may be used selectively; heel lifts and taping may provide temporary offloading or symptom relief. |
Use adjuncts to address defined impairments or barriers, not as substitutes for progressive loading. |
|
Passive modalities |
Low-level laser should not be used; therapeutic ultrasound should not be used alone; night splints remain unsupported. |
Prioritize active rehabilitation and avoid treatment plans centered on low-value passive modalities. |
|
Monitoring and escalation |
Use patient-reported outcomes and performance measures; re-evaluate when recovery is delayed. |
Track VISA-A/TENDINS-A, heel-rise endurance, movement-evoked pain, ROM, strength, and return-to-activity goals; refer when indicated. |
Note. Recommendation grades reflect the article’s evidence hierarchy: A = strong evidence, B = moderate evidence, C = weak evidence, D = conflicting evidence, E = theoretical/foundational evidence, and F = expert opinion.
Reference
Chimenti RL, Neville C, Houck J, Cuddeford T, Carreira D, Martin RL. Achilles pain, stiffness, and muscle power deficits: midportion Achilles tendinopathy revision – 2024: clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health from the Academy of Orthopaedic Physical Therapy of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2024;54(12):CPG1-CPG32. Published online November 27, 2024. doi:10.2519/jospt.2024.0302