Reviewed by: John Baur, PT, DPT, OCS, FAAOMPT
Christiansen and colleagues evaluated whether a telehealth-delivered physical activity behavior change (PABC) intervention could improve real-world activity after unilateral total knee arthroplasty (TKA), an important question because conventional rehabilitation frequently improves impairments and functional test performance without meaningfully changing sedentary lifestyle patterns. The authors framed the study around a clinically relevant gap: many people remain below recommended physical activity levels after TKA, and low activity is associated with poorer mobility, health, and potentially implant-related outcomes. Rather than testing another strengthening or mobility protocol, the trial asked whether rehabilitation should also include a structured self-management strategy designed to change daily behavior. 1
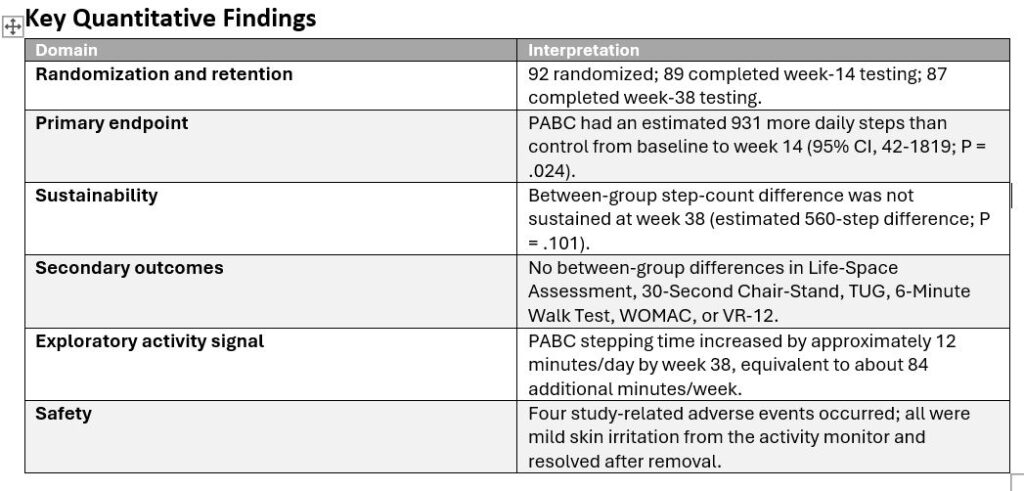
The study was a two-arm, parallel randomized controlled superiority trial conducted within the Veterans Affairs Eastern Colorado Health Care System. Ninety-two U.S. military veterans scheduled for primary unilateral TKA were randomized after returning home from surgery and before beginning conventional outpatient rehabilitation. Participants were 50 to 85 years old, with a mean age in the mid-60s, and the sample was predominantly male (88%), reflecting the VA setting. Randomization was stratified by baseline physical activity level (<5000 versus >=5000 steps/day) and age decade, and outcome assessors were blinded. Both groups received standardized conventional outpatient TKA rehabilitation beginning approximately 2 to 4 weeks after surgery and delivered over 12 sessions tapered across 14 weeks.
The experimental PABC program was layered onto conventional rehabilitation. It consisted of 10 one-to-one telehealth sessions, each 30 minutes, delivered over 12 weeks by trained rehabilitation professionals. Sessions were intentionally tapered: two sessions occurred twice weekly at the start, sessions three through eight occurred weekly, and the final two sessions occurred every other week. Participants were given a wrist-worn Fitbit for daily step-count feedback, while primary outcome measurement used a separate activPAL monitor that did not provide feedback. The behavioral intervention was built around seven linked techniques: education, self-monitoring, tailored feedback, barrier and facilitator identification, problem solving, action planning, and encouragement. Importantly, the intervention shifted from interventionist-led coaching toward participant-led self-management. Action planning used a practical progression target of approximately 3% higher daily steps from the previous week, although goals were tailored to the participant. The attention-control group received telehealth health education sessions matched for frequency and duration, but the content was unrelated to physical activity and included pain management, home safety, diet, medication management, falls, and fractures.
The primary outcome was average daily step count measured with activPAL monitoring during 10-day wear periods at baseline, 8 weeks after surgery, 14 weeks after surgery, and 38 weeks after surgery. The 14-week time point was the primary endpoint. Secondary outcomes included Life-Space Assessment, 30-Second Chair-Stand, Timed Up and Go, 6-Minute Walk Test, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), and Veterans RAND 12-Item Health Survey. Exploratory measures included self-efficacy for exercise and time spent sitting/lying, standing, and stepping. This outcome set is a major strength because it separated physical capacity from free-living behavior, allowing the authors to test whether walking more in daily life followed from improved function or required targeted behavior-change support. 1
The PABC intervention produced a statistically significant short-term improvement in physical activity. From baseline to 14 weeks, the PABC group had an estimated 931 more daily steps than the control group (95% CI, 42-1819; P = .024). Model-estimated daily step counts were similar at baseline (6798 steps/day in both groups), but diverged during rehabilitation: at week 8, the control group averaged 5660 steps/day compared with 6789 in the PABC group; at week 14, the control group averaged 6269 steps/day compared with 7199 in the PABC group. This effect reflects a clinically meaningful behavioral signal, particularly because the control group showed a temporary post-surgical reduction in steps while the PABC group essentially maintained or improved activity through the rehabilitation period. Intervention fidelity was high: PABC fidelity was 97%, control fidelity was 95%, and conventional rehabilitation fidelity was 93%. Fitbit engagement was also strong; all PABC participants reported using the device, and most used it at least daily during the intervention. 1
However, the effect was not sustained at 38 weeks. At follow-up, the PABC group averaged 7345 estimated steps/day compared with 6785 in the control group, a 560-step difference that did not reach statistical significance (P = .101). The absence of a sustained between-group difference is central to interpretation. It suggests that the intervention can shift activity while coaching and feedback are active, but maintenance may require additional booster contacts, peer support, more intensive habit formation strategies, or targeted use among patients with lower baseline activity. The authors also noted that the sample began with relatively high step counts, near 6800 steps/day, and both groups were above 6000 steps/day by 38 weeks. A future trial in patients below 6000 steps/day, or with known psychosocial or environmental barriers, may show a more durable and clinically important effect. 1
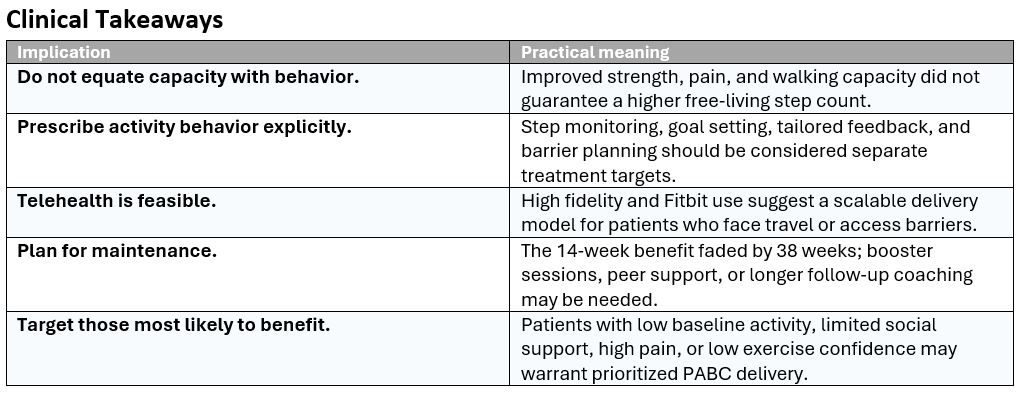
Secondary outcomes improved in both groups but did not differ between groups at either 14 or 38 weeks. This finding is clinically important rather than disappointing. Chair-stand performance, walking capacity, pain, and WOMAC physical function improved with rehabilitation, but those improvements did not automatically translate into greater daily physical activity. The study therefore reinforces a key rehabilitation principle: capacity and behavior are related but not interchangeable. A patient may become stronger, walk farther in a test, and report less pain while still not increasing free-living movement. The PABC model directly addressed that gap by targeting self-efficacy, goal setting, environmental barriers, problem solving, and feedback.
Exploratory findings further support the behavioral interpretation. The PABC group increased observed average daily stepping time from 1.5 hours at baseline to 1.7 hours at week 38, while the control group remained at 1.6 hours. The authors translated the 0.2-hour increase into approximately 84 additional minutes of walking per week. At week 38, the PABC group also spent a greater share of stepping time in longer bouts (>5 minutes) than the control group, suggesting that the intervention may have promoted more purposeful walking rather than only brief household steps. Safety was favorable: four study-related adverse events occurred, all mild skin irritation from the thigh-mounted activity monitor, and no signal suggested increased health care utilization from the intervention.
The trial has several limitations. Generalizability is restricted because the study was conducted in a VA system and included mostly male veterans. The intervention also combined multiple active components, so the study cannot identify whether the most important ingredient was the Fitbit, coaching, motivational interviewing style, action planning, or the overall self-management structure. The PABC design did not include peer social support, despite evidence that peer support can help with goal attainment. Three interventionists were cross-trained across study arms, which creates some possibility of treatment contamination, although fidelity monitoring was strong. Finally, COVID-19 affected in-person testing during the trial, although the authors reported no clear difference in the intervention effect before versus after pandemic onset. 1
Overall, this article provides strong evidence that adding a telehealth self-management intervention to conventional TKA rehabilitation can improve daily physical activity at the end of the intervention, even when functional outcomes are similar between groups. Its most practical message is that post-TKA rehabilitation should not assume improved strength, gait, or pain automatically leads to a more active lifestyle. Clinicians who want patients to move more after TKA may need to prescribe and coach physical activity behavior explicitly, using step monitoring, feedback, goal progression, barrier planning, and self-management strategies. The next step is not merely to prove that PABC works in the short term, but to refine who needs it most and how to sustain the gains beyond the active treatment window.
Visual Synthesis
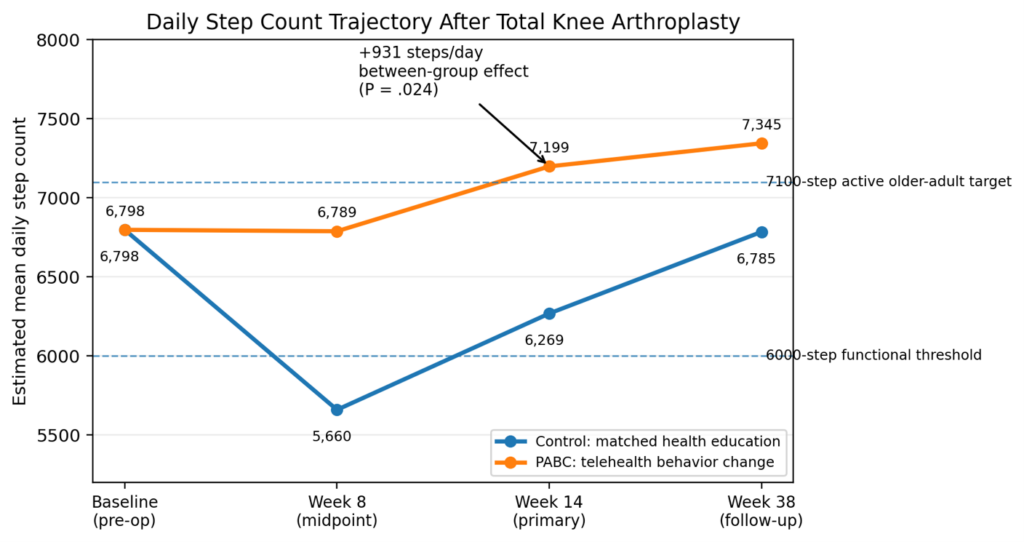
Figure 1. Estimated daily step counts across the TKA rehabilitation timeline. Values are model-estimated means from the article tables; week 14 was the primary endpoint.
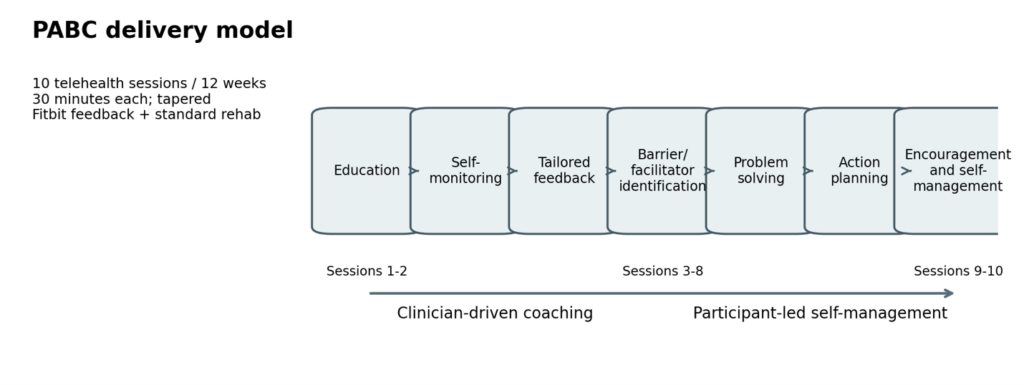
Figure 2. The PABC model combined step-count feedback with behavioral self-management techniques, progressing from clinician coaching to participant-led action planning.
Reference
- Christiansen CL, Kline PW, Anderson CB, Melanson EL, Sullivan WJ, Richardson VL, et al. Optimizing total knee arthroplasty rehabilitation with telehealth physical activity behavior change intervention: a randomized clinical trial. Phys Ther. 2024;104:pzae088. doi:10.1093/ptj/pzae088