Reviewed by: John Baur, PT, DPT, OCS, FAAOMPT
Koc and colleagues present the 2023 revision of the Academy of Orthopaedic Physical Therapy/American Physical Therapy Association clinical practice guideline for heel pain and plantar fasciitis. The article is a focused evidence update intended to help clinicians diagnose, classify, examine, and manage plantar fasciitis within an impairment- and function-based framework. The authors distinguish plantar heel pain as an umbrella term from plantar fasciitis as a more specific clinical entity, emphasizing medial plantar heel pain, tenderness at the medial calcaneal tubercle, and symptoms that are characteristically worse with the first steps after rest or after prolonged weight-bearing.1
The guideline is clinically important because plantar fasciitis is common, often persistent, and frequently seen in both athletic and nonathletic populations. The article notes that plantar fasciitis contributes to approximately 15% of foot pathology in the general population, most often affects adults between 40 and 60 years of age, and may be more common in runners and people whose work requires prolonged standing. Although the term “fasciitis” implies inflammation, the guideline recognizes that the condition may occur along a spectrum that includes inflammatory and degenerative features. This framing is useful because it supports a multimodal plan centered on load management, mobility, tissue tolerance, and function rather than a single inflammatory model.
Methodologically, this revision updates the 2014 clinical practice guideline and concentrates primarily on physical therapist interventions. The authors searched MEDLINE, CINAHL, the Cochrane Library, and PEDro for intervention literature published from December 2012 through March 2023. They graded individual studies by levels of evidence and translated the evidence into recommendation grades ranging from A, reflecting strong evidence, to F, reflecting expert opinion. Risk factors, diagnosis, differential diagnosis, and examination recommendations were largely carried forward from the previous guideline because the authors did not identify new evidence requiring major revisions in those areas. The guideline also explicitly states that it should inform, not replace, individualized clinical judgment and patient preference.
The diagnostic section remains practical and highly usable. Clinicians are encouraged to consider plantar fasciitis when the history and examination show plantar medial heel pain that is most noticeable with initial steps after inactivity, worsens after prolonged weight-bearing, and follows a recent increase in weight-bearing activity. Physical examination findings supporting the diagnosis include pain with palpation of the proximal plantar fascia insertion, a positive windlass test, negative tarsal tunnel tests, limited active and passive talocrural dorsiflexion, abnormal Foot Posture Index-6 findings, and high body mass index in nonathletic individuals. The guideline also highlights risk factors such as limited ankle dorsiflexion, running, and occupational weight-bearing demands, particularly when shock absorption is poor.
The article emphasizes careful differential diagnosis. Clinicians should reconsider the diagnosis or seek consultation when symptoms are inconsistent with plantar fasciitis or fail to improve with appropriate impairment-focused care. Conditions to consider include spondyloarthritis, fat-pad atrophy, proximal plantar fibroma, calcaneal stress fracture, tarsal tunnel syndrome, entrapment of the medial calcaneal nerve or Baxter nerve, S1 radiculopathy, and insertional Achilles tendinopathy. Imaging is usually unnecessary when the clinical presentation is straightforward. If imaging is warranted after failed conservative care or diagnostic uncertainty, the guideline notes that weight-bearing radiographs are generally the first study for chronic foot pain; magnetic resonance imaging without contrast or diagnostic ultrasound may then be considered. Findings such as plantar fascia thickening greater than 4 mm and hypoechoic appearance can support the diagnosis, but imaging abnormalities can be nonspecific and must be interpreted with the clinical picture.
For outcomes and examination, the guideline recommends using validated self-report instruments such as the Foot and Ankle Ability Measure, Foot Health Status Questionnaire, Foot Function Index, and computer-adaptive Lower Extremity Functional Scale. Clinicians should also track reproducible activity limitations and key impairments, including first-step pain, pain with palpation, ankle dorsiflexion range of motion, and body mass index when relevant. The foot and ankle examination outline is broader than a simple heel-pain screen and includes range of motion, joint mobility when deficits are identified, manual muscle testing, heel-raise performance, dorsiflexion lunge testing, Foot Posture Index-6, single-leg squat, gait, balance, special testing, and strategic palpation to assess competing diagnoses.
The strongest intervention recommendations support a multimodal, active, impairment-based plan. Grade A recommendations state that clinicians should use manual therapy directed at lower-extremity joints and soft tissues to address joint and flexibility restrictions, reduce pain, and improve function. Plantar fascia-specific stretching and gastrocnemius/soleus stretching are also strongly recommended for short- and long-term pain reduction and functional improvement. Foot taping, either rigid or elastic, should be used with other physical therapy treatments for short-term improvement in pain and function. Night splints are strongly recommended for a 1- to 3-month period in patients who consistently report first-step morning pain. Importantly, a Grade A negative recommendation states that therapeutic ultrasound should not be used to enhance the benefits of stretching.
Several recommendations are more conditional. Foot orthoses should not be used as an isolated short-term pain-relief treatment, because meta-analyses suggest small to no short-term benefit when orthoses are used alone. However, prefabricated or custom orthoses may be used as part of a combined treatment plan to reduce pain and improve function. Low-level laser therapy has moderate support as part of rehabilitation for short-term pain reduction, while phonophoresis with ketoprofen gel may be used for pain reduction based on weaker evidence. Electrotherapy is positioned as a second-line option; the guideline suggests clinicians may prioritize manual therapy, stretching, and orthoses over electrotherapeutic modalities for short- and long-term outcomes.
The 2023 revision strengthens the role of exercise and dry needling. Clinicians should prescribe therapeutic exercise that includes resistance training for the foot and ankle musculature. Evidence reviewed in the guideline suggests benefit from strengthening programs, heavy-load training, supervised rehabilitation, and multimodal physical therapy that combines education, manual therapy, stretching, resistance training, and neurodynamic interventions. Dry needling to myofascial trigger points in the gastrocnemius, soleus, and plantar foot muscles receives a Grade B recommendation for short- and long-term pain reduction and long-term improvement in function and disability. Reported harms are generally mild, including postneedling soreness and minor bleeding.
Overall, the guideline provides an actionable framework for clinicians managing plantar fasciitis. Its central message is not that one intervention is universally sufficient, but that care should be matched to patient presentation, irritability, impairments, function, and response over time. High-value care prioritizes stretching, manual therapy, taping, symptom-guided night splints, targeted resistance training, load and footwear counseling, and selected adjuncts when appropriate. The main gaps are not whether treatment can help, but which combinations, doses, and sequencing strategies are most effective for specific subgroups of patients. For clinical practice, the article supports a structured approach: confirm the diagnosis, rule out mimics, measure baseline pain and function, apply evidence-supported interventions, reassess regularly, and escalate or consult when recovery is delayed or atypical.
Visual Synthesis
Figure 1. Evidence strength of major intervention statements. A higher grade reflects stronger supporting evidence, not necessarily a stronger “use” recommendation; some high-grade statements are negative recommendations, such as not using therapeutic ultrasound to enhance stretching.
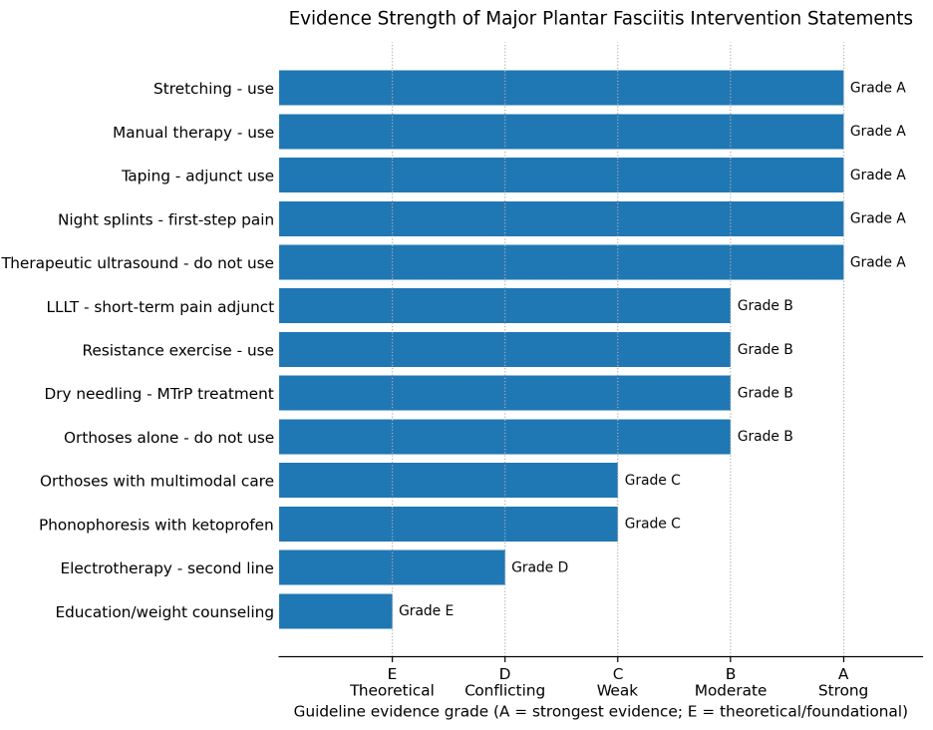
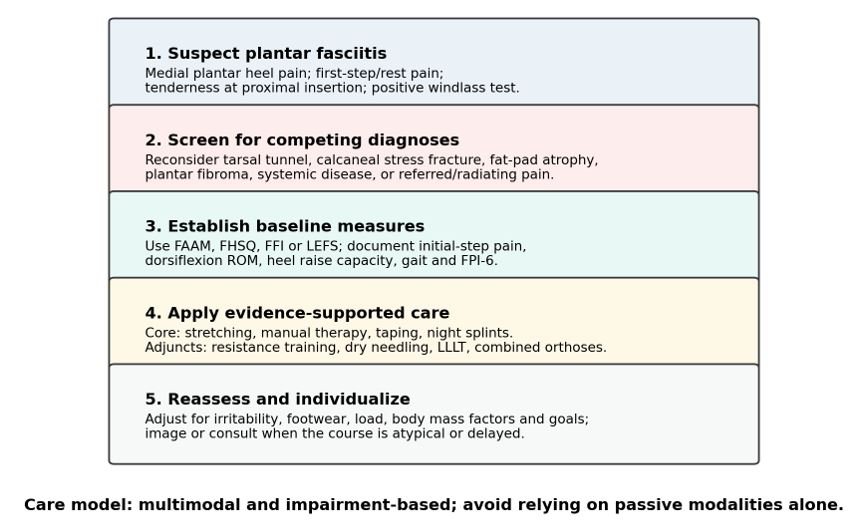
Figure 2. Clinical pathway synthesis derived from the guideline. The figure condenses the article’s decision-making sequence into screening/classification, differential diagnosis, baseline measurement, intervention selection, and reassessment.
Practical Clinical Takeaways
| Clinical Area | Main Recommendation | Grade | Practical Use |
| Diagnosis and screening | Use clinical pattern recognition: plantar medial heel pain, first-step symptoms, palpation pain at the proximal plantar fascia, positive windlass test, and negative tarsal tunnel testing. | B | Rule out mimics when symptoms are atypical or not improving. |
| Core treatments | Use plantar fascia/gastrocnemius-soleus stretching, manual therapy, taping, and targeted night splints. | A | Make these the backbone of conservative care. |
| Orthoses | Do not use orthoses alone for short-term pain; use prefabricated or custom orthoses only with other treatments. | B/C | Most useful as an adjunct when foot posture or taping response supports use. |
| Exercise and loading | Prescribe resistance training for the foot and ankle musculature. | B | Builds local load tolerance and supports long-term self-management. |
| Dry needling | Use for myofascial trigger points in the gastrocnemius, soleus, and plantar foot muscles. | B | Adjunct for pain and disability when clinically indicated. |
| Physical agents | Avoid ultrasound; LLLT may reduce short-term pain; electrotherapy is second line. | A/B/D | Avoid passive modality dominance. |
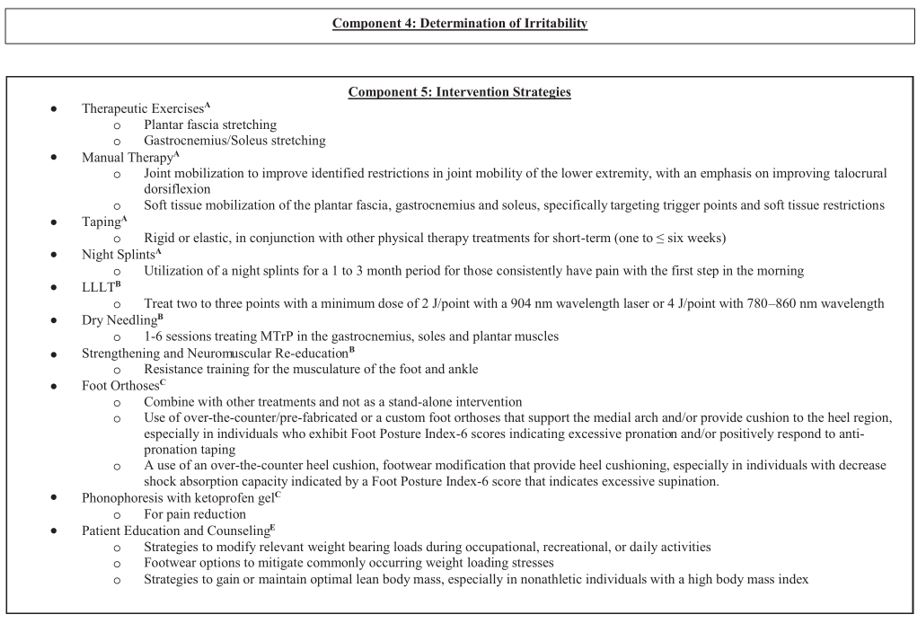
Figure 3. Selected intervention-strategy excerpt from the article’s decision tree (page CPG25). The original guideline states that reproduction and distribution are permitted for educational purposes.
Reference
- Koc TA Jr, Bise CG, Neville C, Carreira D, Martin RL, McDonough CM. Heel pain – plantar fasciitis: revision 2023. J Orthop Sports Phys Ther. 2023;53(12):CPG1-CPG39. doi:10.2519/jospt.2023.0303