Reviewed by: John Baur, PT, DPT, OCS, FAAOMPT
Arundale and colleagues present a 2023 clinical practice guideline (CPG) on exercise-based prevention of knee and anterior cruciate ligament (ACL) injuries. The guideline updates the 2018 recommendations from the Academy of Orthopaedic Physical Therapy and the American Academy of Sports Physical Therapy and links prevention strategies to the International Classification of Functioning, Disability and Health. Its central message is practical and direct: athletes, coaches, parents, and clinicians should use structured, exercise-based injury prevention programs to reduce knee and ACL injuries, particularly in young athletes participating in cutting, pivoting, jumping, and field or court sports.1
The scope is intentionally specific. The authors define exercise-based prevention as active movement by the athlete, including strengthening, stretching, neuromuscular training, proprioceptive work, agility drills, plyometrics, and related training. The guideline excludes passive approaches such as bracing and programs that only provide education. It also excludes broad lower-extremity injury programs unless the intervention specifically targeted knee injury outcomes. This focus strengthens the relevance of the recommendations for physical therapists, athletic trainers, strength and conditioning specialists, physicians, coaches, sports scientists, parents, and athletes who are trying to reduce knee injury burden rather than simply improve general fitness.
Methodologically, the CPG is built on a systematic update of the literature published after the prior guideline. With librarian support, the authors searched PubMed, Scopus, SPORTDiscus, CINAHL, and Cochrane databases, first in October 2020 and again in February 2022. Eligible studies included systematic reviews, meta-analyses, randomized controlled trials, cost-effectiveness studies, and higher-level cohort studies. The team used established appraisal tools, including AMSTAR for systematic reviews, PEDro for randomized trials, and the SIGN checklist for cohort studies. Studies below the quality threshold were not used to develop the recommendations. This process supports the guideline’s emphasis on graded recommendations, with Grade A indicating strong evidence, Grade B moderate evidence, and Grade C weaker evidence.
The strongest conclusion is that exercise-based knee injury prevention programs should be recommended for athletes. Across systematic reviews and meta-analyses, such programs reduce overall knee injuries and ACL injuries specifically. A meta-analysis of eight meta-analyses found a 50% reduction in all ACL injuries and a 67% reduction in noncontact ACL injuries among women athletes. Another meta-analysis of eight randomized or cluster-randomized trials including 13,562 participants found a 53% reduction in ACL injury rates among athletes who participated in injury prevention programs. Programs identified as beneficial include 11+ and FIFA 11, HarmoKnee, Knäkontroll, Prevent Injury and Enhance Performance (PEP), Sportsmetrics, and several protocol-specific interventions evaluated in prior trials.1
The guideline gives particular attention to populations with elevated risk or strong evidence of benefit. Women athletes, especially those younger than 18 years, should participate in exercise-based programs before practices, training sessions, or games. Evidence summarized in the CPG indicates that neuromuscular training reduces ACL injury risk in women athletes from approximately 1 in 54 to 1 in 111, with stronger effects in middle school and high school athletes than in collegiate or professional athletes. Soccer players of both sexes are also a priority group. In male collegiate soccer, FIFA 11+ was associated with a lower ACL injury rate, and in elite men’s soccer, specific training modules reduced severe knee injury incidence from 0.68 to 0.38 injuries per 1000 football exposure hours. The guideline also supports prevention programs for team handball athletes, particularly those aged 15 to 17 years.1
Program content matters. The authors emphasize multicomponent neuromuscular training rather than isolated drills. For women athletes, effective programs should include proximal control exercises, strength training, and plyometric exercises. Hip-focused neuromuscular training is highlighted by a prospective intervention in collegiate women’s basketball, where noncontact ACL injuries were reduced after a program that combined education, hip strengthening, balance, and basketball-specific jump-landing exercises. Balance training may be useful, but the CPG states that balance should not be the only program component. The most clinically useful interpretation is that programs should train the athlete to control the trunk, hip, knee, and lower limb during sport-like tasks that involve acceleration, deceleration, cutting, jumping, and landing.1
The guideline also provides implementation details that are often missing from research summaries. Programs should be performed multiple times per week, last more than 20 minutes per session, and accumulate more than 30 minutes per week. They should begin in the preseason and continue through the regular season. High compliance is essential, particularly among women athletes. In practice, this means the program should be scheduled into routine sport participation rather than treated as optional extra work. Many effective programs are designed as dynamic warm-ups before practice or competition, making them easier to integrate without requiring major additional equipment or clinical time.1
A notable recommendation is that prevention should be implemented broadly among young athletes rather than limited to those identified by screening as high risk. The authors argue that universal implementation better mitigates injury and reduces cost, especially among athletes aged 12 to 25 years in sports with high ACL injury risk, including soccer, basketball, rugby, Australian Rules football, netball, and skiing. Programs may be led by coaches, medical professionals, or both. This is important because the success of injury prevention depends less on knowing that programs work and more on whether teams can deliver them consistently across an entire season.1
The CPG is more cautious about secondary prevention after ACL reconstruction. Based on emerging evidence from the ACL-SPORTS trial, clinicians may recommend exercise-based neuromuscular training in the late phase of ACL reconstruction rehabilitation to reduce the risk of future ACL injury. This recommendation is graded as C, reflecting weaker evidence than the primary prevention recommendations. Nonetheless, the finding is clinically important because second ACL injury risk can be substantial in young athletes returning to cutting and pivoting sports.1
The guideline also identifies important evidence gaps. Most research has been conducted in the United States, northern Europe, and Australia, with limited diversity in athlete populations and limited reporting beyond age and sex. More studies are needed in sports beyond soccer and handball, including basketball, volleyball, netball, skiing, and other high-risk sports. The authors also call for research on alternative delivery models, dose-response relationships, strategies to improve adherence, stakeholder engagement, and emerging approaches such as augmented neuromuscular training, biofeedback, and virtual reality. Overall, the article provides a high-value, practice-ready synthesis: exercise-based knee and ACL injury prevention is effective, inexpensive, low risk, and most powerful when delivered early, repeatedly, and consistently as part of normal sport participation.1
Visual Evidence Synthesis
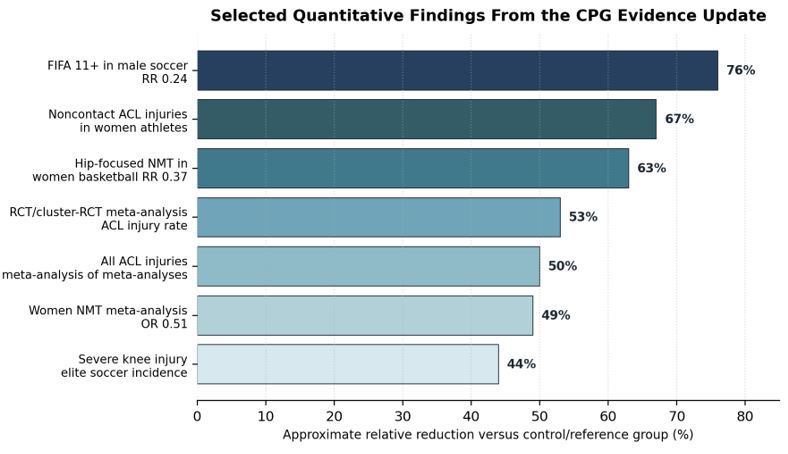
Figure 1. Selected quantitative findings summarized from the guideline evidence update. Percent reductions are orientation estimates derived from reported odds ratios, relative risks, or incidence comparisons and should not be interpreted as directly comparable across populations or study designs.1
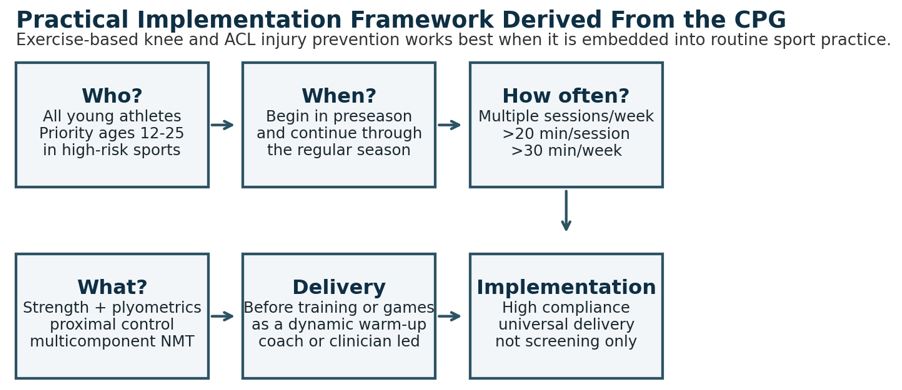
Figure 2. Practical implementation framework derived from the CPG recommendations. The key operational message is to embed neuromuscular training into routine sport participation and monitor compliance throughout the season.1
Key Recommendations and Clinical Interpretation
| Domain | Guideline Recommendation | Clinical Interpretation |
| General athlete population | Recommend exercise-based knee injury prevention programs for prevention of knee and ACL injuries. | Use validated, structured programs such as 11+/FIFA 11, HarmoKnee, Knäkontroll, PEP, Sportsmetrics, or evidence-based protocol variants. |
| Women athletes and youth | Implement programs before practices, training sessions, or games, especially in athletes younger than 18 years. | Prioritize middle school and high school sport settings, where neuromuscular training appears especially protective. |
| Soccer and handball | Soccer players of both sexes and adolescent handball players should use exercise-based prevention programs. | Build sport-specific warm-ups into team routines; target jumping, landing, cutting, trunk control, and lower-limb alignment. |
| Program content | Use multicomponent programs with strength, plyometrics, and proximal control; balance alone is insufficient. | Train movement quality under sport-like demands rather than relying on isolated static balance exercises. |
| Dose and timing | Train multiple times per week, longer than 20 minutes per session, and more than 30 minutes per week. | Start in preseason and continue through the regular season; dose and repetition are central to effectiveness. |
| Implementation strategy | Implement broadly among all young athletes, not only those screened as high risk. | Universal delivery can reduce missed cases and improve cost-effectiveness in high-risk sports. |
| Secondary prevention | Late-phase neuromuscular training after ACL reconstruction may help prevent future ACL injury. | Useful during return-to-sport preparation, but the evidence is weaker than for primary prevention. |
Table 1. Summary of key clinical practice recommendations and practical implications.1
Reference
- Arundale AJH, Bizzini M, Dix C, et al. Exercise-Based Knee and Anterior Cruciate Ligament Injury Prevention: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability and Health From the Academy of Orthopaedic Physical Therapy and the American Academy of Sports Physical Therapy. J Orthop Sports Phys Ther. 2023;53(1):CPG1-CPG34. doi:10.2519/jospt.2023.0301