Reviewed by Jerome Thomas, SPT, Tyler Tice, PT, DPT, OCS, ATC
Achilles tendinopathy is a very common, overuse injury of the lower extremity that often affects athletes and highly-active individuals that engage in activities such as running, jumping, and other recreational-related tasks. Achilles tendinopathy can consequently become detrimental to a patient’s activity levels and overall functional capacity as many patients may begin to decrease their activity in response to pain or decline in function. There are a very limited number of randomized controlled trials and established treatment protocols for Achilles tendinopathy, despite various forms of modalities and exercise utilized for this patient population. This prospective, randomized controlled trial attempted to evaluate the efficacy of utilizing the Pain-Monitoring Model in combination with a continued, tendon-loading training regimen for patients with Achilles tendinopathy.
In this study, 38 patients with Achilles Tendinopathy were divided into two separate treatment groups: an exercise training group (n=19) and an active rest group (n=19) that was not allowed to perform any physical activity for the first 6 weeks of rehabilitation. However, both treatment groups were rehabilitated with an identical, progressive Achilles tendon-loading program for 12 weeks to 6 months. As previously mentioned, the exercise training group was allowed to continue loading activities for the Achilles tendon in accordance with the Pain-Monitoring Model in the same timeframe that the active rest group was restricted .
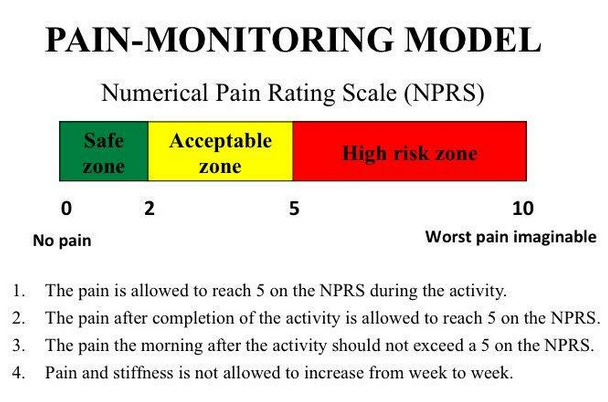
Guidelines for the Pain-Monitoring Model were modified by Silberngael et al. in their 2001 study. According to their guidelines for the pain-monitoring model, pain was not allowed to reach level 5 on the VAS where a 0 indicated no pain and a 10 indicated the worst pain imaginable. Pain after the exercises were allowed to reach a 5 on the VAS but should have subsided by the following morning. Additionally, pain and stiffness in the Achilles tendon were not allowed to increase from week to week. Treatment protocol consisted of a progressive, four-phase program that incorporated the following exercises: 2-legged, 1-legged, eccentric, and fast-rebounding toe raises. Phase 3 allowed the patients to transition to more plyometric-style movements if the subsequent phases were handled with no pain in the tendon insertion or increased morning stiffness. The primary outcomes utilized for the conclusion of this randomized controlled trial were the VISA-A-S score, which was a specialized Achilles assessment questionnaire, as well as pain with hopping measured with the VAS scale.
The results of the trial showed that both treatment groups showed significant improvements in VISA-A-S score and hopping pain in comparison to baseline measurements at 6 weeks, 3 month, 6 month, and 12 month evaluations. More importantly, this study could not demonstrate any negative findings or implications for allowing the patients in the exercise training group to continue Achilles tendon-loading activities in accordance with the Pain-Monitoring Model. Therefore, early implementation of strengthening exercises for the Achilles tendon and plantar flexor complex, as well as moderated activities such as running and jumping, can be utilized to reduce symptoms and improve functional capacity in patients with Achilles tendinopathy. In previous literature, it had been recommended that patients with Achilles tendinopathy take a rest period from the activities that were pain-provoking. However, this study demonstrates that those same activities can be continued as long as the patient with Achilles tendinopathy is following the protocols set by the Pain-Monitoring Model.
Clinical Application:
Based on this study, we can use the Pain Monitoring Model as a guide to help determine the appropriate amount of activity and exercise for the proper amount of loading to the Achilles tendon with Achilles tendinopathy without “overdoing it”. Below is a graphic that simplifies the explanation of this model:
Reference:
Silbernagel KG, Thomeé R, Eriksson BI, Karlsson J. Continued sports activity, using a pain-monitoring model, during rehabilitation in patients with Achilles tendinopathy: a randomized controlled study. Am J Sports Med. 2007 Jun;35(6):897-906. doi: 10.1177/0363546506298279. Epub 2007 Feb 16. PMID: 17307888.