by Ray Moore, PT, DPT, OCS
The purpose of this capstone project was to describe the case of a patient who presented to the clinic with an uncommon motor neuron disease including the treatment plan and discussion of orthopaedic manual therapy principles. Benign calf amyotrophy is a sub category of lower motor neuron diseases often called benign focal amyotrophy. This condition was originally reported by Hirayama et al. (Cintas 2017) and focused on Asian male youth with distal upper extremity muscle atrophy and weakness. Lower extremity involvement was later reported as Wasted Leg Syndrome by Prabhakar et al. in 1981. Since, several forms and presentations of benign focal amyotrophy have been studied and reported on yet there remains a gap between empirical studies and clinical treatment. Relative to other motor neuron disorders such as ALS and myopathies, little is known of the etiology, cause and treatment of benign focal amyotrophy. Some reports indicate that fewer than one hundred cases involving the lower extremity have been diagnosed, with most in the eastern hemisphere, particularly India. Consequently, this author was unable to locate significant research pertaining to physical therapy or other treatment of benign calf amyotrophy (Cintas 2017).
There are two proposed origins leading to benign focal amyotrophy: repetitive trauma and idiopathic cause. The available literature notes that males are considerably more affected, up to 10:1 male to female ratio, and most patients are under the age of 30 at diagnosis (Cintas 2017). There is some variability of age range in different parts of the world which has led some to believe that benign focal amyotrophy is a diverse condition with varying types of presentations. The earlier upper extremity variant described by Hirayama was believed to be caused by repetitive cervical spine flexion trauma or microtrauma causing flattening of the cord. 
However, MRI of the lumbar spine of patients with lower extremity involvement are typically normal with no cord or nerve root abnormalities detected (Cintas 2017). However, MRI showed “marked atrophy and increased signal intensity were found mainly in gastrocnemius and soleus muscles” in one study (Hamano 1999). EMG is one of the most helpful diagnostic tools and findings include “fibrillations, positive sharp waves and fasciculations” (Cintas 2017). Nerve conduction velocity can be normal or slowed. 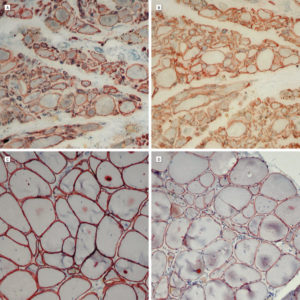
(Stain of normal gastrocnemius cells vs. muscle cells in BCA, Felice et al. 2003)
Other signs indicative of lower motor neuron involvement can be present including hyporeflexia, absent Babinski sign, visible atrophy, calf muscle fasciculations, and fatigable weakness. Surrounding musculature is typically spared such as foot intrinsics however Hamano et al. reported involvement of some quadriceps and hamstring muscles in one patient (Hamano 1999). To date, there is no clear explanation for the predominant involvement of the gastroc-soleus muscles.
A key difference between benign focal amyotrophy and other motor neuron diseases is the lack of progression and self-limiting nature. Patients with benign calf amyotrophy experience lower leg weakness over a period of months to years which can last for a variable period. Most reports suggest that lower leg weakness and atrophy slowly worsens then stabilizes. Due to the lack of long term studies, it is unclear whether patient experience a full return of muscle strength, girth and function once the progression has ceased. Treatment for severe upper extremity cases can include avoidance of cervical spine flexion, cervical collar use, and cervical spine surgery with duroplasty (Cintas 2017). A search for treatment of lower extremity or benign calf amyotrophy revealed no empirical studies other than a brief mention of physical and occupational therapy. Given the lack of findings on lumbar MRI versus cervical and upper extremity involvement, novel functional treatment approaches must be discovered.
Case Presentation
The patient, referred to as Robert, presented to our clinic and was referred by a neurologist with a special interest in neuromuscular disorders and EMG. He is a 28 year old male of Greek origin who began experiencing gradual right calf weakness about one year prior to this evaluation. Robert reported no trauma or known change in activity level prior to symptom onset. He also experienced right lateral foot numbness which did not progress. Prior to this evaluation, Robert reported some left lateral foot numbness but states that this fully resolved. Robert’s right calf weakness progressed over several months and six months later he began seeing his neurologist. At this point, Robert reported visible right calf atrophy compared to the left. His neurologist ordered lumbar spine MRI with and without contrast which was unremarkable and EMG/NCV testing. Robert’s NCV testing was normal bilateral but needle EMG showed fibrillation potentials and positive sharp waves in the right medial gastrocnemius muscle and to a lesser degree in the tibialis posterior. There were no motor unit action potentials of the right gastrocnemius and reduced recruitment of the tibialis posterior. Additionally, Robert’s serum creatine kinase was elevated at 596 U/L. 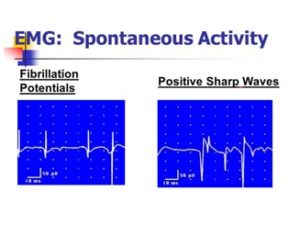
On examination, Robert is a tall and physically fit individual who was previously an avid runner. Robert is a school teacher and waited six months after seeing his neurologist to schedule a PT appointment due to his schedule. Upon PT evaluation, the primary diagnosis was a suspected S1 nerve root lesion and benign calf amyotrophy was not mentioned on his PT prescription. He reported no history of pain and Robert demonstrated abbreviated stance on right lower extremity during gait with limited toe push off in end stance phase.
Robert’s right mid-calf muscle girth measured two cm less than the left and his right Achilles deep tendon reflex was absent while all other lower extremity reflexes were within normal limits. Sensation to light touch was normal except diminished over right lateral 5th metatarsal. Lumbar and lower extremity range of motion was normal, straight leg raise and slump tests negative, and Babinski/clonus were absent. Small, infrequent fasciculations were detected in the right gastrocnemius and ankle plantarflexion was measured at 3+/5 compared to 5/5 on the left. All other lower extremity MMT was 4+/5 to 5-/5 and normal for his age.  Of note, there was minimal palpable contraction of the right gastroc-soleus during resisted plantarflexion. No significant lumbar or other orthopaedic abnormalities were found during the examination. Robert was instructed in some lower extremity therapeutic exercises and we attempted to finish the session with Russian muscle stimulation to the right gastroc. Interestingly, Russian stimulation was unable to evoke muscle activation or twitch response from Robert’s gastroc-soleus, though he did feel increasing tingling sensation, a finding I had not previously seen in eight years of experience.
Of note, there was minimal palpable contraction of the right gastroc-soleus during resisted plantarflexion. No significant lumbar or other orthopaedic abnormalities were found during the examination. Robert was instructed in some lower extremity therapeutic exercises and we attempted to finish the session with Russian muscle stimulation to the right gastroc. Interestingly, Russian stimulation was unable to evoke muscle activation or twitch response from Robert’s gastroc-soleus, though he did feel increasing tingling sensation, a finding I had not previously seen in eight years of experience.
At a subsequent follow up visit, Robert reported that he had seen his neurologist to review findings and she suspected he had benign calf amyotrophy, which is often a diagnosis of exclusion once other neuromuscular pathologies are ruled out. Since I was not previously aware of this rare condition, I researched the topic thoroughly to best provide a treatment plan for my patient and quickly found a lack of evidence or even non-empirical discussion. While benign focal amyotrophy is a self-limiting lower motor neuron disease, it is still possible to positively affect a patient’s outcome and quality of life with orthopaedic manual therapy and other physical therapy interventions.
Treatment and Research
Erl Pettman discusses the facilitated segment and its impact on extremity strength (NAIOMT 2005). In this article, Pettman details how acute or repetitive injuries leading to segmental stiffness can cause additional unexpected outcomes. Facet hypomobility at a segment can cause an adjacent or nearby hypermobility. For example, limited left hip spin can lead to lack of left hip extension and/or rotation. For normal gait to occur, this individual will have to hyperextend a segment in the lumbar spine or sacroiliac joint to allow upright gait. Similarly, an L3 hypomobility into extension may lead to an extension hypermobility at L4 or L5 to promote full normal lumbar extension during functional movement. When this issue becomes sub-acute to chronic, abnormal segmental input to the segment occurs which can present with both changes locally and in the extremities (Pettman 2005).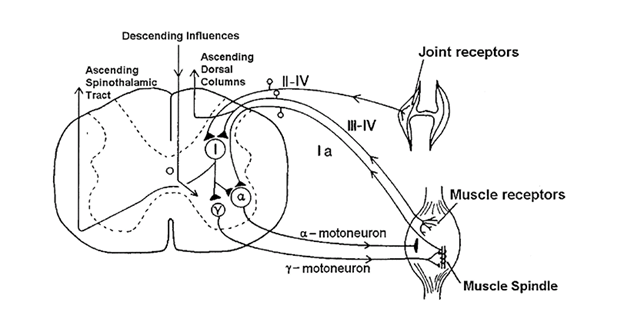 Segmental facilitation can cause muscle tenderness, hypo or hyperreflexia, altered skin and muscle sensitivity, muscle hypertonicity, inhibition of antagonist muscle groups, and muscle weakness that it typically not fatigable. Pettman discusses common segmental facilitation at C2/3, C5/6 and L4/5, though it can occur at any spinal segment. “It is proposed that the constant afferent barrage ultimately leads to a state of ‘central segmental excitation’ that, in turn, lowers the synaptic resistance and facilitates neuronal transmission” (Pettman 2005). Furthermore, as discussed throughout the lab courses in the Fellowship program, manual therapy treatment to the axial spine can be beneficial in improving peripheral signs and symptoms.
Segmental facilitation can cause muscle tenderness, hypo or hyperreflexia, altered skin and muscle sensitivity, muscle hypertonicity, inhibition of antagonist muscle groups, and muscle weakness that it typically not fatigable. Pettman discusses common segmental facilitation at C2/3, C5/6 and L4/5, though it can occur at any spinal segment. “It is proposed that the constant afferent barrage ultimately leads to a state of ‘central segmental excitation’ that, in turn, lowers the synaptic resistance and facilitates neuronal transmission” (Pettman 2005). Furthermore, as discussed throughout the lab courses in the Fellowship program, manual therapy treatment to the axial spine can be beneficial in improving peripheral signs and symptoms.
One of the hallmark examples discussed by Pettman is the treatment of C5/6 for tennis elbow caused in part by segmental facilitation (Pettman 2005). Manipulations, mobilizations, proprioceptive mobilizations, muscle energy techniques, and proprioceptive neuromuscular facilitation can improve the afferent barrage that this segment is receiving and reduce the peripheral consequences of that segment. One such benefit of these treatments is the increase of peripheral myotomal muscle strength.
In a randomized controlled trial, Chilibeck et al. tested the effects of spinal manipulation on imbalances in lower extremity strength (Chilibeck 2011). These authors performed segment specific chiropractic manipulations on subjects found to have a 15% or higher strength discrepancy between lower extremities. Chilibeck et al. performed manipulations and placebo treatment to the spinal level associated with the muscle that they found weakness. For example, subjects with hip flexor weakness received treatment to the corresponding L2-3 level. This study found that lumbar spine manipulation can lead to a statistically significant increase in strength in knee and hip flexion for individuals with 15% or greater difference in pre-treatment strength. The authors discuss possible explanations for increased lower extremity strength following spinal manipulation including “reduced nerve impingement, altered discharge from muscle spindles, Golgi tendon organs, mechanoreceptors and nocioceptors, altered sensory processing in the spinal cord, and altered skeletal muscle reflexes….to cause an increase in motor neuron excitability” (Chilibeck 2011). This can lead to improved motor unit firing and increased strength in the associated myotome.
Robert’s mechanical lumbar exam did not show any significant instabilities, hypomobility, or considerable tenderness. Robert was limited in thoracic-lumbar junction right rotation and demonstrated hypermobility into right extension at L5-S1 as measured by PPIVM, PAIVM and H/I testing. Robert’s end-range was excessive but pain free. For this reason, a thoraco-lumbar junction manipulation was performed followed by neuro-muscular re-training to this level. Robert’s right rotation immediately improved but hypermobility was still noted at L5-S1. While it was understood that the cause of Robert’s right calf weakness was clearly not restricted to the musculoskeletal system (given his negative lumbar MRI and other findings), it was hypothesized that some deficits may be caused by segmental facilitation at L5-S1, or that the minor mechanical lesions in the lumbar spine were a result of altered gait pattern due to neuropathic gastroc-soleus weakness.
Following the thoracic-lumbar junction manipulation, proprioceptive wobble PA mobilizations were performed at L5/S1 to improve afferent inputs with the possibility of increasing some gastroc-soleus strength that was limited by potential segmental facilitation versus motor neuron pathology. Given the self-limiting nature of the patient’s diagnosis, it was explained that any additional safe method to increase his lower extremity strength would be worth a trial. After two treatment sessions, the patient reported about 10% improvement in his right lower extremity strength with weight bearing activities and he began to demonstrate a slight observable and palpable contraction of his gastroc-soleus muscle upon voluntary contraction.
An early indication that Robert’s condition was not limited to the musculoskeletal system was his response to Russian current muscle electric stimulation. Following his initial evaluation, I and a colleague attempted to apply muscle stimulation to Robert’s gastroc-soleus. Using multiple currents and variations of parameters, we were unable to elicit a single twitch response. The patient was able to feel the current sensation but no muscle contraction. After reviewing Michelle Cameron’s Physical Agents in Rehabilitation, I found that “denervated muscles do not contract in response to the pulses of electricity that produce contractions in innervated muscles” since the “current causes depolarization of their motor nerves” (Cameron 2003). At this time, I hypothesized that this patient was experiencing a condition related to pathologic denervation. Cameron mentions that denervated muscles can be stimulated by “long pulses of electricity, lasting for 10 ms or longer.” The typical treatment for denervated muscle is direct current stimulation however research has shown that any effect may be related to placebo and DC stimulation could hinder nerve regeneration (Cameron 2003). Therefore, I did not continue with muscle electric stimulation. However, in retrospect, I may have considered Russian muscle stimulation to the lumbar multifidus for the same reasoning as mobilization/manipulation for segmental facilitation.
Much of this patient’s treatment consisted of therapeutic exercise as well as a home exercise program. Initially, Robert performed de-weighted calf raises in the seated position, single leg stance to tolerance with one hand assist, and theraband exercise for tibialis posterior strengthening. Robert performed 3-4 sets of 20 repetitions for endurance training or he performed exercises to fatigue. Robert was instructed to allow additional rest between sets for 45-60 seconds due to the fatigability of his lower extremity muscles.
Since Robert was an avid runner and weightlifter prior to this condition, his exercise routine included functional activities with modifications made as necessary. Robert was unable to perform standing de-weighted bilateral heel raises, but after two sessions, he was able to complete sets of heel raises on the leg press on the lowest resistance. Robert also performed bilateral leg press until he was able to complete weight bearing squats without excessive left trunk lean. Resistance for the leg press was set based on Robert’s subjective ability to perform repetitions without heavily relying on the left lower extremity. Robert also performed stool scoots early with right leg for activation of neighboring musculature.
Emphasized throughout the Fellowship didactic and lab work is the role of the individual spinal segmental stabilizers, like the multifidus, and their role in global stabilization and mobility. Much like a train, if each car is not properly connected and stabilized, the entire train will not move. If the multifidus and other segmental stabilizers do not properly stabilize a segment, such as L5-S1, then the entire mechanics of the spine can be affected and locomotion and functional mobility is not optimal. For this reason, specific activation of the L4-S1 multifidus, as well as transverse abdominis and kegel exercises were implemented. Robert was instructed on multifidus step-down activation with tactile cues. Transverse abdominis and kegel muscle activation was added and more advanced exercises were built from this foundation. Robert was encouraged to include segmental stabilizer activation in all static and dynamic activities of his daily routine.
After two sessions, Robert was able to progress to balance and higher level strengthening activities such as single leg dead lift with one hand assist, balance activities on soft surface, and hopping on trampoline on right leg. Advanced balance and strengthening exercises such as plantarflexion and dorsiflexion on foam board and double leg squats on bosu ball were added at subsequent visits. On the fourth visit, I saw Robert in the evening and he complained of lower leg swelling. He stated that it was improving but he still experienced swelling in the evening. Due to lack of function of the muscle pump, I provided Robert with a lower leg sleeve to be worn on days that he would be in the dependent position. Additionally, since Robert is a teacher, I suggested that Robert take seated or supine rest breaks whenever possible and perform ankle pumps. These modifications helped to reduce Robert’s complaints of lower leg swelling in the evening.
By his sixth visit, Robert reported about 25% improvement in right lower leg strength and 50% or more improvement in overall functional improvement since initial evaluation. He was demonstrating a palpable and observable contraction of his gastroc-soleus and had progressed to exercises like right SLS on trampoline with soccer ball kick and the slide board for agility. While Robert was unable to return to running, he was much more confident in his gait and did not experience tripping over his right foot. Robert then had a follow up visit with his neurologist and left the country for a two week vacation.
When he returned three weeks later, Robert reported that he was being referred to another hospital for work up and treatment for benign calf amyotrophy. He reported that while on vacation, he did not get to perform his home exercise program or other exercise much and stated that his right lower leg strength improvements had diminished. However, functionally, Robert felt that he had made considerable improvements in physical therapy and reported improved confidence following treatment. Robert was resuming teaching the following week and stated that he would have to self-discharge due to time restrictions. Robert had a follow up EMG study that showed “some firing” compared with little to no activity prior. He was able to voluntarily contract his gastroc-soleus with visible contraction during exercises. Robert still complained of mild sensory deficit over the lateral foot but stated that it had improved since beginning physical therapy. Robert’s right calf girth increased by one centimeter in a six week period. Robert reported that he had experienced the most progress in over a year while he participated in physical therapy. Robert was discharged with the recommendation that he follow up as his schedule allowed to continue to improve any remaining functional deficits.
Discussion
As expert clinicians, we are expected to be able to treat both simple and complex cases, perform detailed yet directed evaluations, demonstrate pattern recognitions, and have a wealth of knowledge of conditions to perform differential diagnosis. However, the knowledge and preparation an expert clinician should possess cannot be limited or contained in a box. Often, clinicians are forced to adapt to new information on unforeseen exposure. In this case, a patient with a motor neuron disease that is so uncommon that very few in the physical therapy field are aware of it, came to my clinic with an atypical presentation. Having performed the lumbar and lower extremity scan many times, I was quickly able to recognize that this patient did not show the normal signs and symptoms of radiculopathy or lumbar pathology.
Furthermore, I determined that this patient probably did not exhibit an atypical presentation of a common condition. For example, while receiving mentoring during this Fellowship, my mentor and I evaluated a patient with lateral thigh pain. While I hastily suspected the lumbar spine, I learned about a potential entrapment point for the lateral femoral cutaneous nerve just above the iliac crest. Like much of the valuable knowledge and experience I had gained during mentorship, I was previously unaware of this entrapment site. Still, I was able to recognize that this patient could have an atypical presentation of a common condition. This Fellowship Program also furthered my ability to recognize patients that require attention outside of the scope of physical therapy practice. Had Robert come to our clinic as a direct access patient, I would have immediately referred him to a physician.
Since Robert was under a physician’s care and he presented with functional impairments from an undiagnosed condition, I used my training to develop an individualized treatment plan for Robert both before and after his diagnosis was confirmed. The expert clinician may be occasionally challenged by an unfamiliar diagnosis or presentation. Fellowship and other training can assist in making that clinician adaptable to apply previously learned material and experiences to the creation of a treatment plan for a new diagnosis.
The particular difficulty that this case provided was a lack of clinical or empirical evidence for treatment of benign focal amyotrophy. Several searches uncovered some literature that mentions the words physical and occupational therapy, but little other treatment was specified. One might assume that since self-limiting, individuals with benign focal amyotrophy do not require physical therapy. However, physical therapy is a critical component in the recovery of people diagnosed with Guillaine-Barre Syndrome and other self-limiting diseases. Physical therapy is not limited to conditions that it is the primary treatment of choice such as whiplash or tennis elbow.
Conclusion
This capstone project involves the application of skills and knowledge possessed by a Fellow in training to a topic not previously highlighted in physical therapy literature. Limitations included the lack of considerable literature, especially pertaining to treatment, and a sample size of one patient. While preparing for this capstone project, one intervention I would have implemented was muscle stimulation to the lumbar multifidus. Still, it was a very valuable experience to treat a patient with such a rare condition and assist in his progress and regaining of functional mobility. It is often difficulty for a young and active patient to understand their condition and why they can’t perform at the level they were accustomed. As a physical therapist, part of our job is to help return that function to the best of our ability and provide understanding and education for the patient. Both before and after confirmed diagnosis, Robert appreciated the education he was provided and he fully bought into his treatment plan. He showed some progress which was uncertain given his diagnosis. Fortunately for me, Robert presented to my clinic after I have performed much of the requirements for Fellowship training, including mentoring hours. While my mentor did not specifically prepare me to treat someone with benign calf amyotrophy, I was prepared to adapt and care for a patient with a condition that I could not reasonably be trained for, which I believe is one of the chief purposes of Fellowship training.
References:
- Cintas, P. (2017). Motor neuron diseases: Benign focal amyotrophy. Revue Neurologique, 173(Motor neuron diseases), 338-344. doi:10.1016/j.neurol.2017.03.016
- Felice K, Whitaker C, Grunnet M. Benign calf amyotrophy: clinicopathologic study of 8 patients. Archives Of Neurology [serial online]. October 2003;60(10):1415-1420.
- Hamano T, Mutoh T, Kuriyama M, et al. MRI findings of benign monomelic amyotrophy of lower limb. Journal Of The Neurological Sciences [serial online]. June 1, 1999;165(2):184-187.
- Chilibeck P, Cornish S, Schulte A, et al. The effect of spinal manipulation on imbalances in leg strength. The Journal of the Canadian Chiropractic Association. September, 2011; 55(3): 183-192.
- Pettman, E. The Facilitated segment. The North American Institute of Orthopaedic Manual Therapy. October, 2005; Volume IX, Issue 5.
- Cameron, M. Physical Agents in Rehabilitation: From Research to Practice (Second Edition). Saunders.