Reviewed by: John Baur, PT, DPT, OCS, FAAOMPT
Teichert and colleagues conducted a systematic review and meta-analysis to update the evidence on whether exercise interventions prevent new episodes of neck pain in adults without neck pain at baseline. The topic is clinically important because neck pain is common, recurrent, and burdensome in both personal and occupational settings. The article emphasizes that neck pain ranks behind only low back pain among musculoskeletal disorders for years lived with disability, and office workers are a particularly relevant population because annual incidence in that group has been reported as 20% to 50%. Existing clinical practice guidelines have historically focused more on treatment than prevention, leaving uncertainty about whether proactive exercise programs should be implemented before symptoms occur.1
The authors built their review around a focused clinical question: in adults from the general population who were not experiencing neck pain at baseline, do exercise interventions reduce the occurrence of a subsequent neck pain episode compared with no intervention, placebo or sham, attention control, or minimal intervention such as advice or education? Military personnel and astronauts were excluded because their exposure profiles and occupational demands differ substantially from the general population. Eligible interventions included any physical exercise approach judged to be the main part of the intervention. This broad definition allowed inclusion of strength or resistance exercise, stretching, motor control exercise, general physical activity, and combined exercise programs.
The methods were rigorous and reflect contemporary standards for systematic reviews. The authors searched MEDLINE, Embase, CENTRAL, CINAHL, SPORTDiscus, PEDro, ClinicalTrials.gov, and the WHO International Clinical Trials Registry Platform from inception through December 2, 2022. They also performed forward and backward citation searches and contacted authors and experts to identify potentially missed studies. Randomized controlled trials, including cluster randomized trials, were eligible if they followed participants for at least 3 months and reported the occurrence of one or more neck pain episodes. Risk of bias was assessed with the Cochrane RoB 2 tools, and certainty of evidence was judged using the GRADE framework. The meta-analysis used random effects methods, adjusted cluster randomized trials for clustering, and included sensitivity analyses for intracluster correlation assumptions, alternative outcome definitions, adjusted trial estimates, and missing outcome data.
Five trials were included in the meta-analysis. Across these studies, 1,722 participants were randomized at baseline, although the pooled analysis was based on 1,340 participants available at the latest follow-up. The follow-up period ranged from approximately 5 to 12 months. Most participants were office workers, with one study including laboratory technicians; overall, the pooled population was best characterized as workers with primarily static or repetitive occupational demands. The mean participant age was approximately 40 years, and most participants were women. The exercise interventions varied: two trials used resistance programs focused on the neck and shoulder muscles, one trial used stretching combined with motor control exercise, one trial used a walking-based physical activity intervention with financial incentives, and one trial used an individually tailored program in which many participants performed strength and cardiovascular exercise. Comparators were no intervention or minimal intervention, and one trial provided a brief ergonomic assessment to both groups.
The main finding was that exercise interventions probably reduce the risk of a new neck pain episode in the short term, defined as 12 months or less. The pooled odds ratio was 0.49 with a 95% confidence interval of 0.31 to 0.76, indicating that the odds of developing neck pain were about half as high in exercise groups as in control groups. The authors translated this into absolute terms using an assumed 12-month comparator risk of 30%. Under that assumption, approximately 300 of 1,000 people performing mainly static work would be expected to develop neck pain without exercise, compared with about 173 of 1,000 with preventive exercise. This corresponds to 127 fewer cases per 1,000 people, with a number needed to treat of approximately 8 to prevent one episode over 12 months. The absolute benefit changes with baseline risk; at lower baseline risk, the benefit is smaller, while higher-risk populations may experience larger absolute risk reduction.
Despite the favorable pooled estimate, the authors appropriately avoid overstating the findings. The certainty of evidence was rated as moderate, not high, primarily because of study limitations and risk of bias. No trial was judged to be at low overall risk of bias. Two trials had some concerns, and three were rated at high risk of bias, largely because of missing outcome data. The sensitivity analyses for missing data were especially important: when plausible assumptions were made that missing participants in intervention groups may have been more likely to develop neck pain, the confidence interval became compatible with trivial effects. This does not negate the main result, but it lowers confidence in the precision and stability of the effect estimate.
The review has several notable strengths. It updated a prior evidence base that had likely overestimated the preventive effect because of a small number of studies and less robust analytic methods. It included newly published trials, adjusted cluster trials for clustering, used more conservative meta-analytic methods, and provided absolute risk differences that are more clinically interpretable than relative estimates alone. The authors also shared data and statistical code, increasing transparency and reproducibility. These features make the review more trustworthy than earlier summaries of the same question.
The limitations are equally important for clinical interpretation. The body of evidence is small, and most trials were conducted in office or work-related settings, so generalizability to physically demanding occupations, community populations, or people recently recovered from neck pain remains uncertain. Exercise programs were heterogeneous, preventing firm conclusions about the best type, dose, supervision model, or adherence strategy. Outcome definitions varied across trials, and outcomes were self-reported, which is difficult to avoid in prevention studies but still introduces measurement concerns when participants cannot be blinded. The authors also note that harms, costs, health care utilization, sick leave, and productivity were not sufficiently studied, even though those outcomes matter when recommending interventions to people who are currently asymptomatic.
For clinicians, the practical message is that preventive exercise is reasonable to recommend, particularly for office workers and people exposed to prolonged static postures or repetitive computer-based tasks. The findings support the use of exercise as a low-risk preventive strategy, but not as a precisely defined protocol. A pragmatic program might include neck and shoulder strengthening, movement breaks, stretching or motor control work, and general physical activity, selected according to patient preference, work demands, and adherence likelihood. The estimated benefit should be discussed in absolute terms, because patients and employers may judge the value of prevention differently depending on baseline risk, required time, cost, equipment, and tolerance for temporary soreness.
The authors conclude that exercise interventions probably reduce the short-term risk of new neck pain episodes, but whether the range of possible effects is worthwhile should be decided through individualized discussion. Future research should use standardized definitions of a neck pain episode, prospectively registered protocols, better reporting of exercise interventions, careful cluster trial methods, more complete follow-up, and systematic monitoring of adverse events and economic outcomes. Studies should also test strategies to improve adherence and evaluate populations beyond office workers. Overall, the article provides a strong argument for considering exercise-based prevention while maintaining appropriate caution about uncertainty, implementation details, and clinical significance.
Figures and Clinical Interpretation
Figure 1 translates the pooled odds ratio into expected absolute benefit at several plausible baseline risks. Higher baseline risk produces a larger absolute benefit and a lower number needed to treat (NNT).
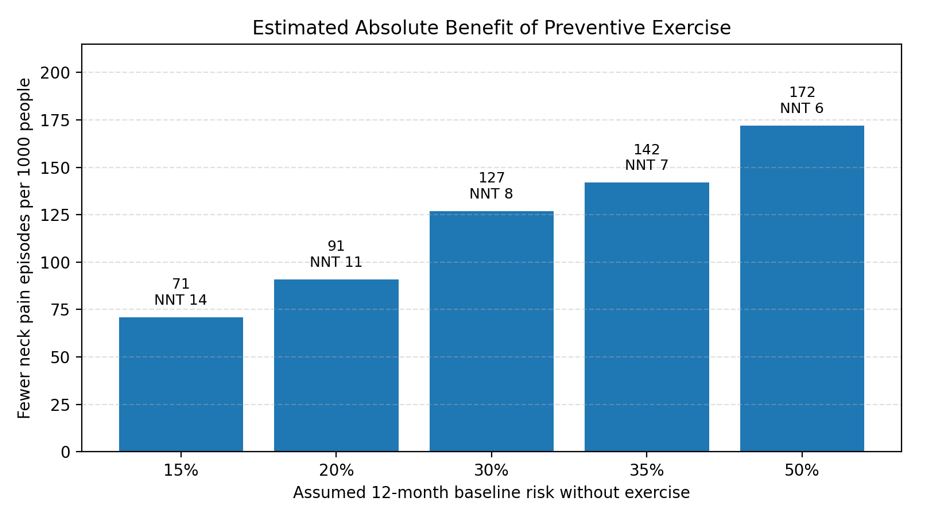
Figure 1. Estimated absolute benefit based on the pooled OR of 0.49 and Table 4 assumptions from the article. NNT = number needed to treat.
Figure 2 reproduces the article’s forest plot of the pooled trial results. The overall effect favors exercise, but the range of trial estimates and the authors’ missing-data sensitivity analyses support cautious interpretation.
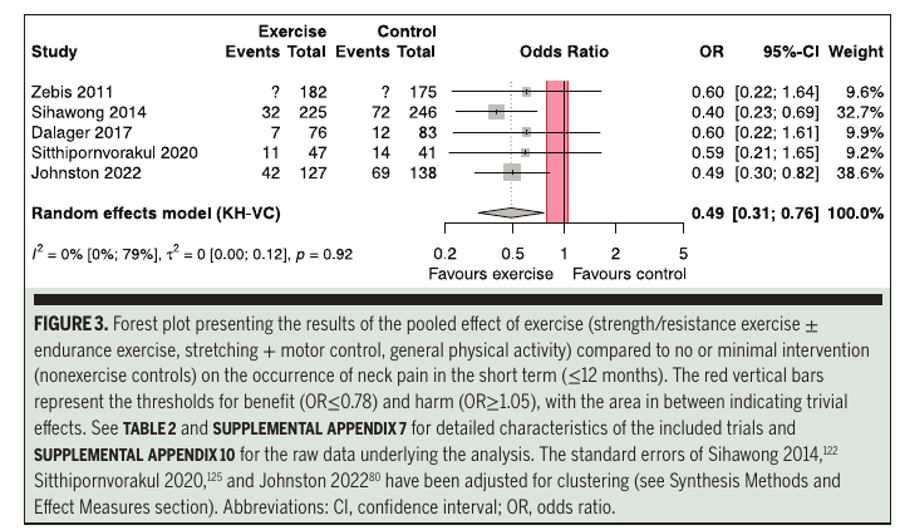
Figure 2. Forest plot of exercise versus no or minimal intervention for short-term neck pain prevention. Reproduced from Teichert et al.
Practical Clinical Takeaways
|
Clinical area |
Implication |
Practice note |
|
Best-supported population |
Workers with mostly static or repetitive demands, especially office workers. |
Do not assume the same benefit for all occupations or community populations. |
|
Intervention choice |
Evidence supports exercise broadly, not one superior protocol. |
Use feasible options such as neck/shoulder strengthening, stretching, motor control work, walking, and movement breaks. |
|
Expected effect |
At 30% baseline risk, approximately 127 fewer episodes per 1,000 people over 12 months were estimated. |
Frame benefit in absolute terms; NNT was approximately 8 at this assumed baseline risk. |
|
Confidence |
Evidence was moderate certainty and not robust to all missing-data assumptions. |
Discuss uncertainty and monitor adherence, symptom response, and tolerability. |
|
Implementation |
Programs should be easy to perform repeatedly and integrated into daily routines. |
Workplace programs may benefit from leadership support, reminders, and brief supervised instruction. |
|
Research gaps |
Harms, cost-effectiveness, productivity, sick leave, and optimal dose remain uncertain. |
Future trials should use standardized episode definitions and better follow-up. |
Reference:
- Teichert F, Karner V, Döding R, Saueressig T, Owen PJ, Belavy DL. Effectiveness of exercise interventions for preventing neck pain: a systematic review with meta-analysis of randomized controlled trials. J Orthop Sports Phys Ther. 2023;53(10):594-609. doi:10.2519/jospt.2023.12063